

Impact of autoantibody status on stratifying the risk of organ involvement and mortality in SSc: experience from a multicentre French cohort of 1605 patients
- PMID: 39572073
- PMCID: PMC11580297
- DOI: 10.1136/rmdopen-2024-004580
Impact of autoantibody status on stratifying the risk of organ involvement and mortality in SSc: experience from a multicentre French cohort of 1605 patients
Abstract
Introduction: Systemic sclerosis (SSc) is a rare autoimmune disease currently classified into two subgroups based on skin extension. The aim of this study was to determine in a large cohort whether the determination of autoantibody (AAb) profile among a full antinuclear AAbs panel including nine specificities had a higher impact than skin phenotype on stratifying the risk of organ involvement and mortality in SSc.
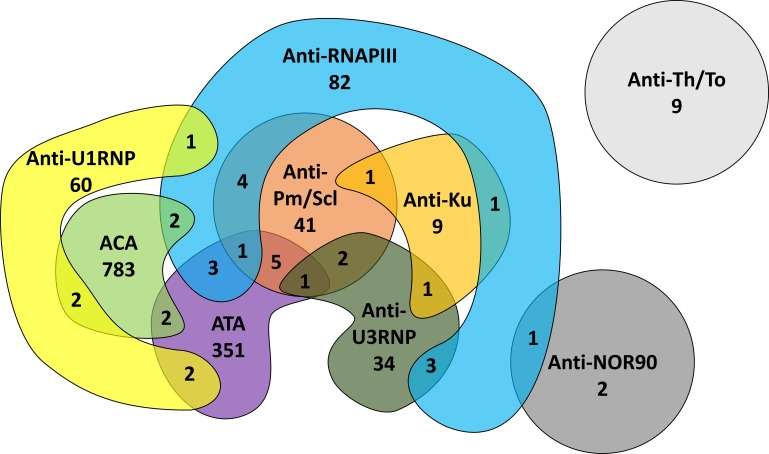
Methods: Data for patients with SSc followed in seven French university hospitals were retrospectively analysed in terms of skin phenotype, AAbs (anti-topoisomerase I (ATA), anticentromere (ACA), anti-RNA polymerase III (anti-RNAPIII), anti-U1RNP, anti-U3RNP, anti-Pm/Scl, anti-Ku, anti-Th/To, anti-NOR90), organ involvement and mortality. Multivariate analyses were performed to identify independent factors associated with organ involvement and mortality.
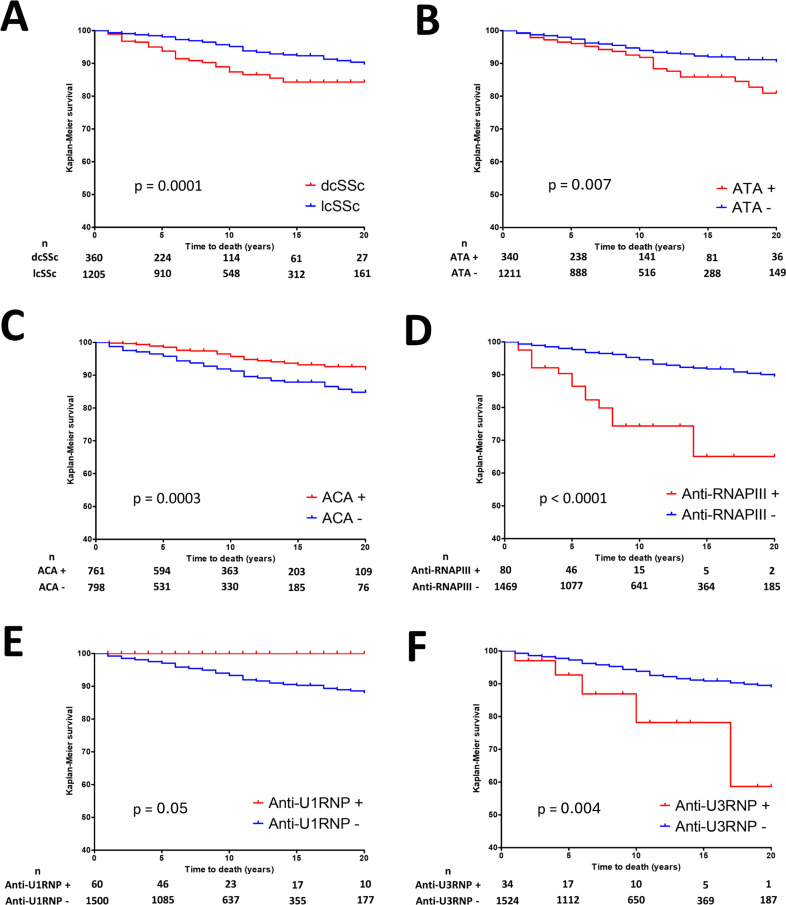
Results: We included 1605 patients with SSc (367 with diffuse cutaneous SSc). On multivariate analysis, ATAs were associated with interstitial lung disease and mortality (OR=3.27 (95% CI 2.42 to 4.42); HR=1.9 (95% CI 1.01 to 3.58)), anti-RNAPIII with scleroderma renal crisis and mortality (OR=7.05 (95% CI 2.98 to 16.72); HR=2.35 (95% CI 1.12 to 4.93)), anti-U1RNP with arthritis (OR=3.79 (95% CI 2.16 to 6.67)), anti-Pm/Scl and anti-Ku with myositis (OR=7.09 (95% CI 3.87 to 12.98) and 7.99 (95% CI 2.41 to 26.46)). The skin phenotype was not associated with survival or organ involvement on multivariate analysis without stepwise selection.
Conclusion: This study unravels, by contrast with skin phenotype, a strong association between AAbs specificities, organ involvement and outcome in SSc and suggests that patients' classification based on only skin extension is not sufficient for defining prognosis and phenotype.
Keywords: autoantibodies; classification; mortality; systemic sclerosis.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- LeRoy EC, Medsger TA. Criteria for the classification of early systemic sclerosis. J Rheumatol. 2001;28:1573–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous