

Spontaneous multilevel lumbar pediculolysis associated with spondylolysis: a rare case and review of the literature
- PMID: 39574019
- PMCID: PMC11580524
- DOI: 10.1186/s12891-024-08084-8
Spontaneous multilevel lumbar pediculolysis associated with spondylolysis: a rare case and review of the literature
Abstract
Background: Pediculolysis is bone hypertrophy and pseudoarthrosis caused by pedicle fracture and has often been combined with contralateral spondylolysis in previous reports. Multilevel pediculolysis with spondylolysis is extremely rare, and we report a case who underwent surgery. Cases of multisegment pediculolysis were reviewed to inspire the diagnosis and treatment of similar pathological phenomena.
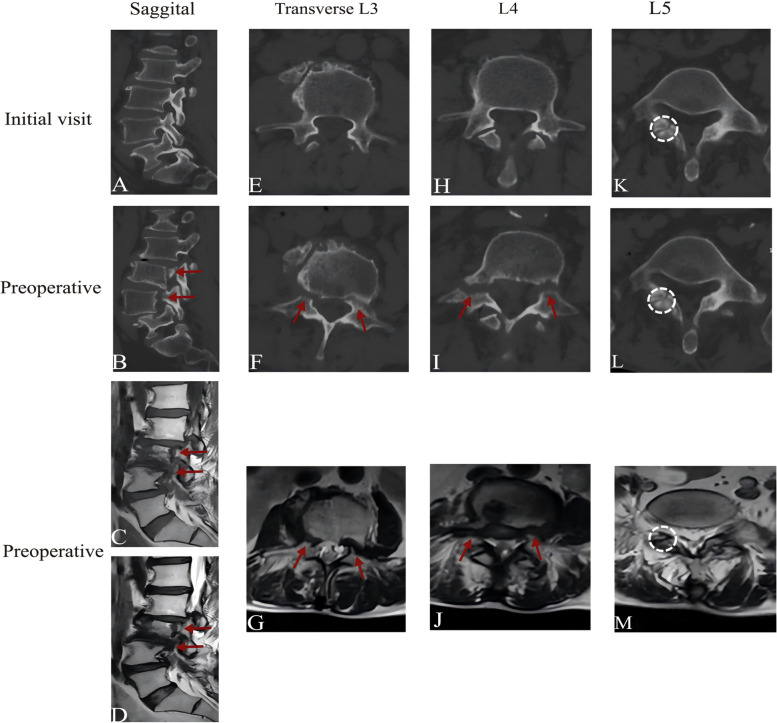
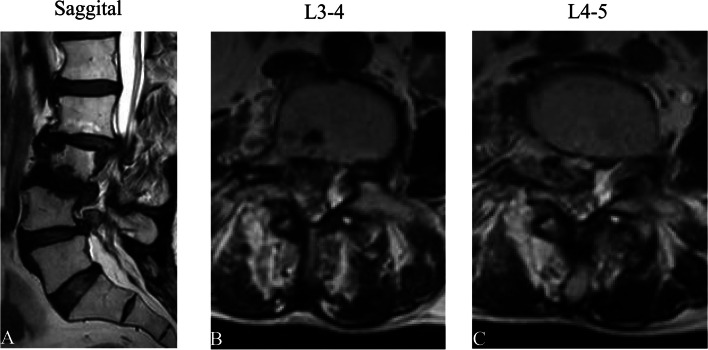
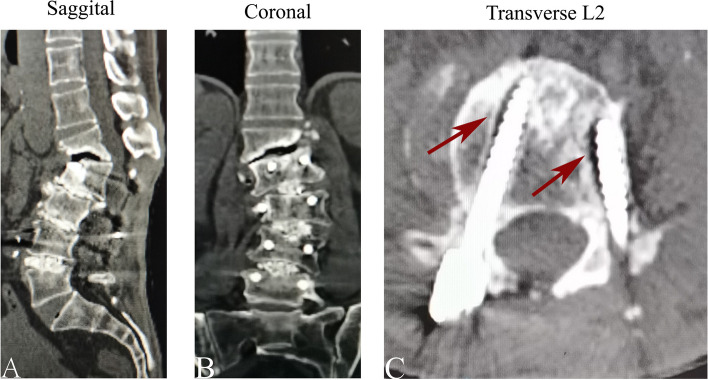
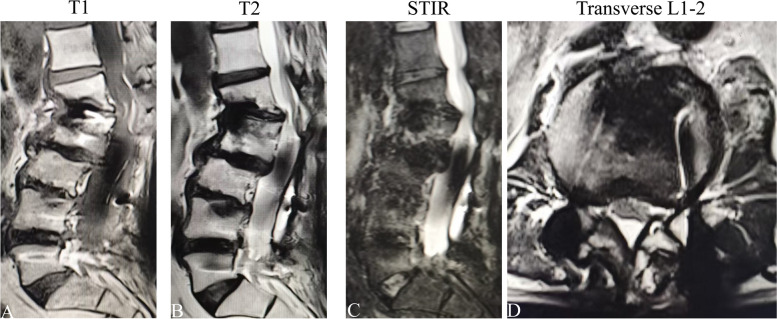
Case presentation: A 55-year-old man suffering from low back pain and sciatica was admitted to hospital after failing conservative treatment. The imaging studies revealed bilateral pediculolysis at L3 and L4 and right spondylolysis at L5. When L2-5 internal fixation and fusion surgery were performed, the symptoms improved immediately after surgery. At the 2-year postoperative follow-up, proximal junctional failure appeared and progressively worsened.
Conclusions: Multilevel pediculolysis often requires surgical intervention, and segment instability is an important consideration in the development of surgical fusion strategies. The etiology of pediculolysis is still complex and unknown, and the spondylolysis protocol can be used as a reference for treatment. Surgeons should be cautious in surgical planning to minimize the likelihood of postoperative instrumentation failure.
Keywords: Global spinopelvic balance; Pediculolysis; Proximal junctional kyphosis; Spondylolysis; Surgical intervention.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Approval for this study was obtained from the Ethics committee of the Affiliated Hospital of Southwest Medical University(KY2024400). Consent for publication: Informed consent was obtained from participating researchers to publish information and images. The patient provided written informed consent to release personal and clinical details and all identifying images. This paper has not been published elsewhere in whole or in part, or submitted elsewhere for review. All authors have read and approved the content. Competing interests: The authors declare no competing interests.
Figures



Similar articles
-
Unilateral spondylolysis combined with contralateral lumbar pediculolysis in a military parachutist.J Spinal Disord Tech. 2006 Feb;19(1):65-7. doi: 10.1097/01.bsd.0000161230.87271.f3. J Spinal Disord Tech. 2006. PMID: 16462222
-
Symptomatic Unilateral Pediculolysis Associated with Contralateral Spondylolysis and Spondylolisthesis in Adults-Case Report and Review of Literature.World Neurosurg. 2020 Nov;143:339-345. doi: 10.1016/j.wneu.2020.08.055. Epub 2020 Aug 11. World Neurosurg. 2020. PMID: 32795684
-
A rare case of non-traumatic, multi-level, bilateral pedicle fractures of the lumbar spine in a 60-year-old patient.Eur Spine J. 2017 May;26(Suppl 1):197-201. doi: 10.1007/s00586-017-5029-3. Epub 2017 Mar 16. Eur Spine J. 2017. PMID: 28303382
-
Double-level lumbar spondylolysis and spondylolisthesis: A retrospective study.J Orthop Surg Res. 2018 Mar 16;13(1):55. doi: 10.1186/s13018-018-0723-3. J Orthop Surg Res. 2018. PMID: 29548343 Free PMC article. Review.
-
Non-traumatic lumbar spondylolysis with contralateral pedicle and lamina fracture: a case report and review of the literature.BMC Musculoskelet Disord. 2025 Jan 14;26(1):48. doi: 10.1186/s12891-025-08293-9. BMC Musculoskelet Disord. 2025. PMID: 39810096 Free PMC article. Review.
References
-
- Ekin EE, Altunrende ME. Pedicle Stress Injury in Children and adolescents with Low Back Pain. Spine (Phila Pa 1976). 2019;44(17):E1038–44. - PubMed
-
- Gunzburg R, Fraser RD. Stress fracture of the lumbar pedicle. Case reports of pediculolysis and review of the literature. Spine (Phila Pa 1976). 1991;16(2):185–9. - PubMed
-
- Wiener MD, Martinez S, Forsberg DA. Congenital absence of a cervical spine pedicle: clinical and radiologic findings. AJR Am J Roentgenol. 1990;155(5):1037–41. - PubMed
-
- Wilkinson RH, Hall JE. The sclerotic pedicle: tumor or pseudotumor? Radiology. 1974;111(3):683–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
