

Antihypertensive Treatment Patterns in CKD Stages 3 and 4: The CKD-REIN Cohort Study
- PMID: 39574792
- PMCID: PMC11577237
- DOI: 10.1016/j.xkme.2024.100912
Antihypertensive Treatment Patterns in CKD Stages 3 and 4: The CKD-REIN Cohort Study
Abstract
Rationale & objective: Blood pressure (BP) control is essential for preventing cardiorenal complications in chronic kidney disease (CKD), but most patients fail to reach BP target. We assessed longitudinal patterns of antihypertensive drug prescription and systolic BP.
Study design: Prospective observational cohort study.
Setting & population: In total, 2,755 hypertensive patients with CKD stages 3-4, receiving care from a nephrologist, from the French CKD-Renal Epidemiology and Information Network (CKD-REIN cohort study).
Exposure: Patient factors, including sociodemographic characteristics, medical history, and laboratory data, and provider factors, including number of primary care physician and specialist encounters.
Outcomes: Changes in antihypertensive drug-class prescription during follow-up: add-on or withdrawal.
Analytical approach: Hierarchical shared-frailty models to estimate hazard ratios (HR) to deal with clustering at the nephrologist level and linear mixed models to describe systolic BP trajectory.
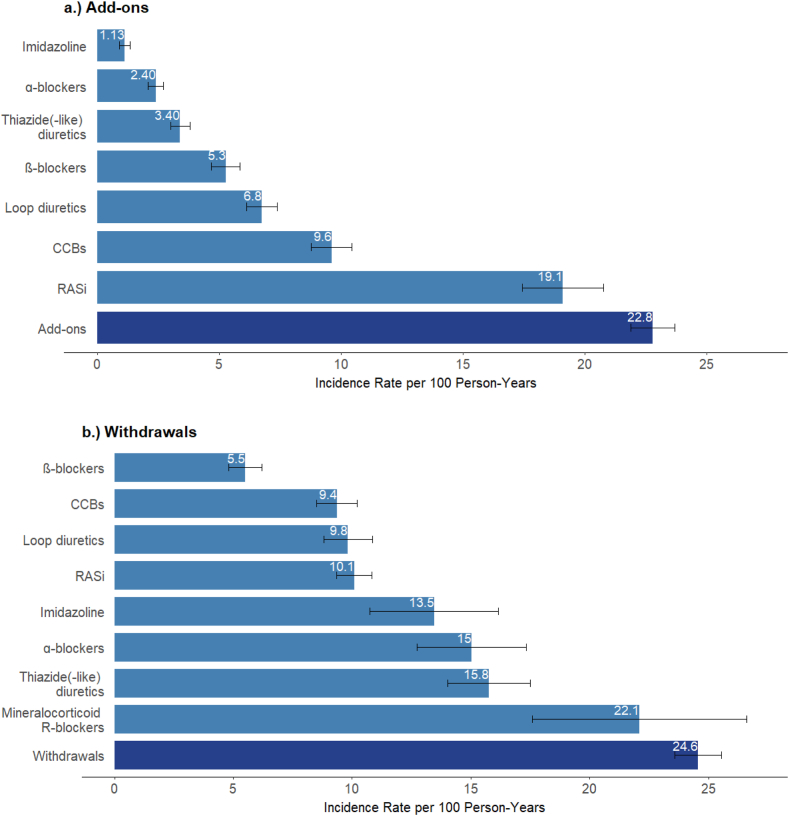
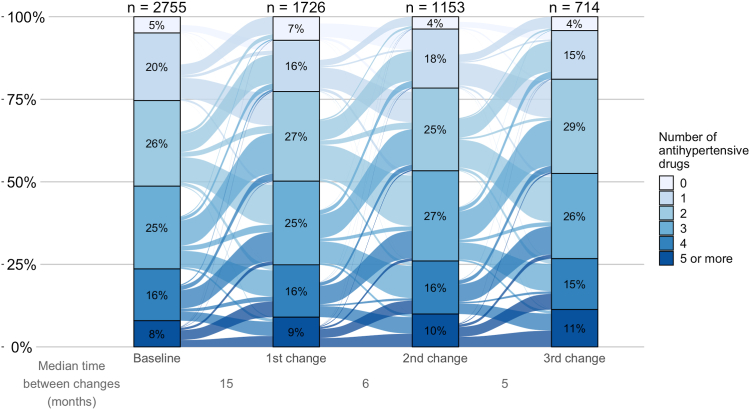
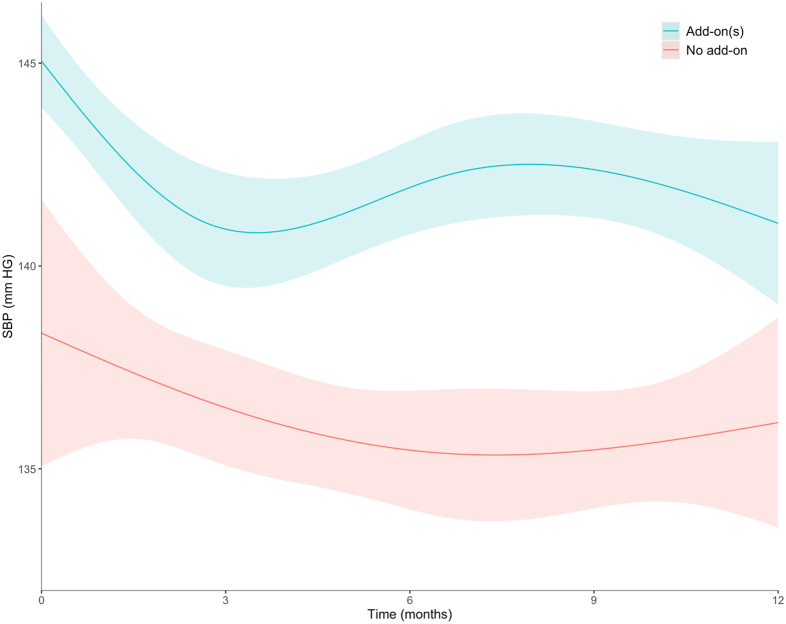
Results: At baseline, median age was 69 years, and mean estimated glomerular filtration rate was 33 mL/min/1.73 m². In total, 66% of patients were men, 81% had BP ≥ 130/80 mm Hg, and 75% were prescribed ≥2 antihypertensive drugs. During a median 5-year follow-up, the rate of changes of antihypertensive prescription was 50 per 100 person-years, 23 per 100 for add-ons, and 25 per 100 for withdrawals. After adjusting for risk factors, systolic BP, and the number of antihypertensive drugs, poor medication adherence was associated with increased HR for add-on (1.35, 95% confidence interval [CI], 1.01-1.80), whereas a lower education level was associated with increased HR for withdrawal (1.23, 95% CI, 1.02-1.49) for 9-11 years versus ≥12 years. More frequent nephrologist visits (≥4 vs none) were associated with higher HRs of add-on and withdrawal (1.52, 95% CI, 1.06-2.18; 1.57, 95% CI, 1.12-2.19, respectively), whereas associations with visit frequency to other physicians varied with their specialty. Mean systolic BP decreased by 4 mm Hg following drug add-on but tended to increase thereafter.
Limitations: Lack of information on prescriber and drug dosing.
Conclusions: In patients with CKD and poor BP control, changes in antihypertensive drug prescriptions are common and relate to clinician preferences and patients' tolerability. Sustainable reduction in systolic BP after add-on of a drug class is infrequently achieved.
Keywords: antihypertensive agents; blood pressure; chronic kidney disease; hypertension; renin-angiotensin system.
Plain language summary
Blood pressure (BP) control remains unattained in most patients with chronic kidney disease (CKD), raising questions about how antihypertensive treatment is managed. Our study highlights dynamic, yet heterogeneous patterns of antihypertensive drug prescriptions in patients with CKD stages 3-4 receiving care from a nephrologist over 5 years of follow-up. Modifiable factors such as high body mass index and poor medication adherence were associated with higher hazard of adding-on an antihypertensive drug class, independently of baseline BP and antihypertensive treatment. Similarly, lower education level was associated with antihypertensive drug withdrawn, as was more frequent visits to primary care physicians, underlining the importance of coordinated care. Sustainable reduction in systolic BP after add-on of a drug class is infrequently achieved and may be related to drug withdrawal and poor treatment adherence.
© 2024 The Authors.
Figures
References
-
- Ku E., Lee B.J., Wei J., Weir M.R. Hypertension in CKD: core curriculum 2019. Am J Kidney Dis. 2019;74(1):120–131. - PubMed
LinkOut - more resources
Full Text Sources
