

This is a preprint.
Severe motor impairment is associated with lower contralesional brain age in chronic stroke
- PMID: 39574865
- PMCID: PMC11581069
- DOI: 10.1101/2024.10.26.24316190
Severe motor impairment is associated with lower contralesional brain age in chronic stroke
Abstract
Background: Stroke leads to complex chronic structural and functional brain changes that specifically affect motor outcomes. The brain-predicted age difference (brain-PAD) has emerged as a sensitive biomarker. Our previous study showed higher global brain-PAD associated with poorer motor function post-stroke. However, the relationship between local stroke lesion load, regional brain age, and motor impairment remains unclear.
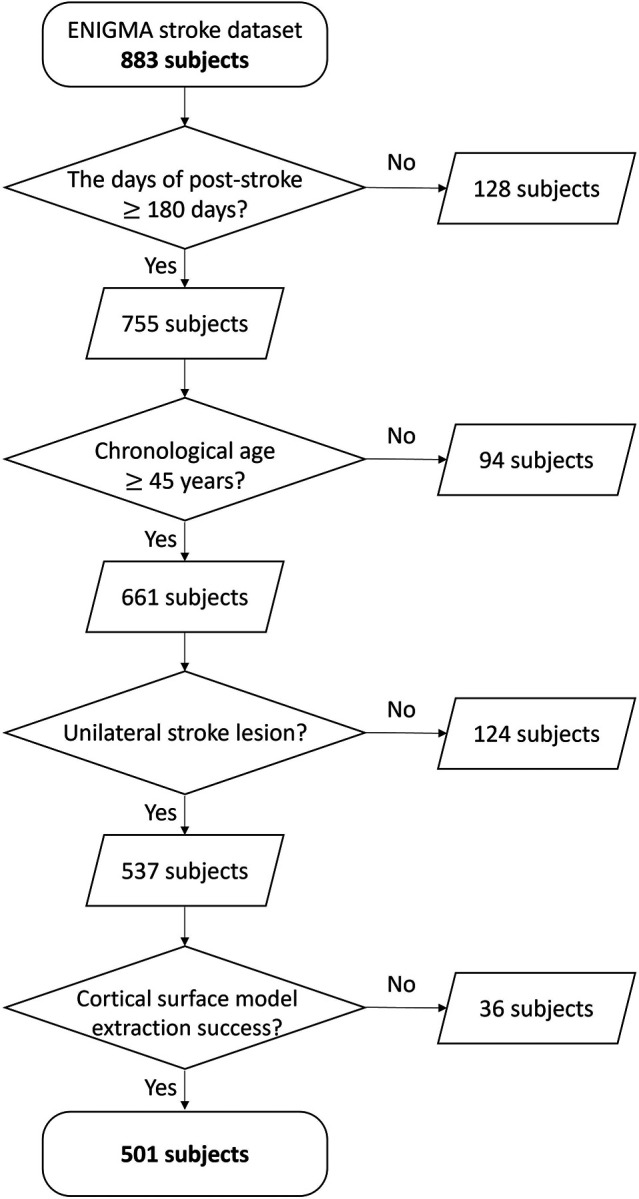
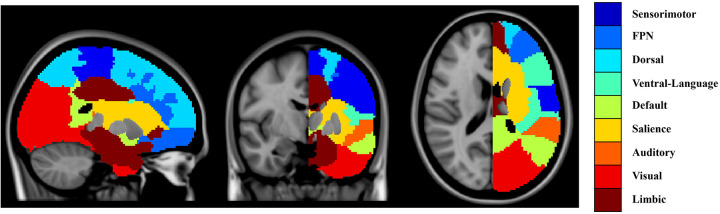
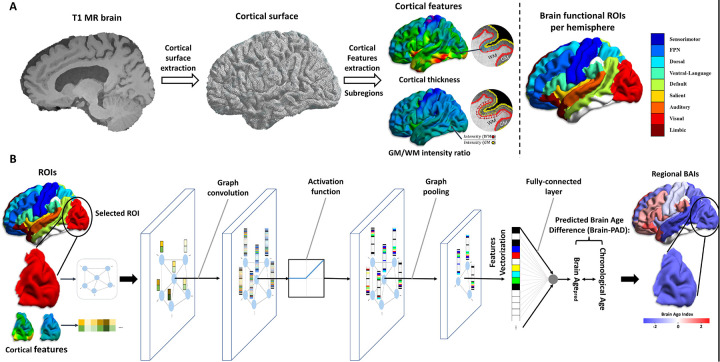
Methods: We studied 501 individuals with chronic unilateral stroke (>180 days post-stroke) from the ENIGMA Stroke Recovery Working Group dataset (34 cohorts). Structural T1-weighted MRI scans were used to estimate regional brain-PAD in 18 predefined functional subregions via a graph convolutional network algorithm. Lesion load for each region was calculated based on lesion overlap. Linear mixed-effects models assessed associations between lesion size, local lesion load, and regional brain-PAD. Machine learning classifiers predicted motor outcomes using lesion loads and regional brain-PADs. Structural equation modeling examined directional relationships among corticospinal tract lesion load (CST-LL), ipsilesional brain-PAD, motor outcomes, and contralesional brain-PAD.
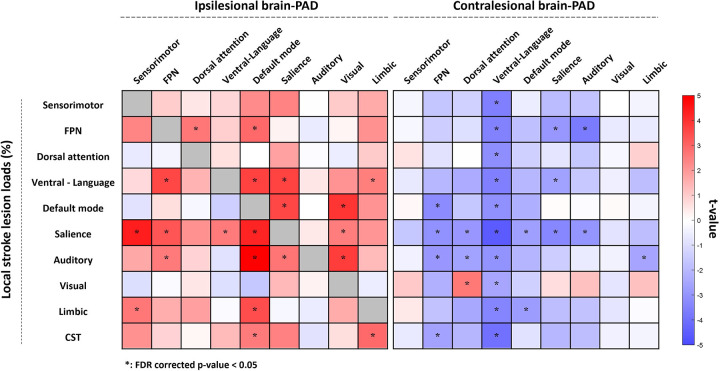
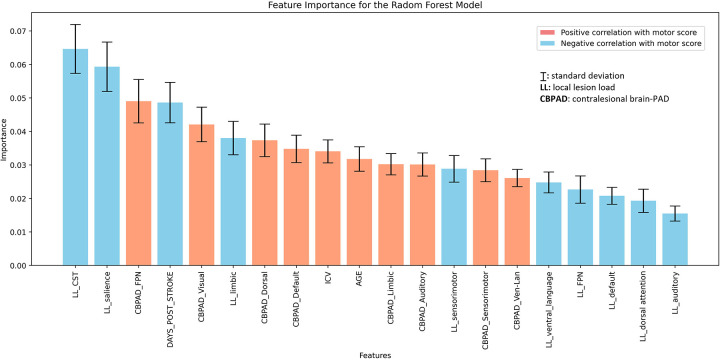
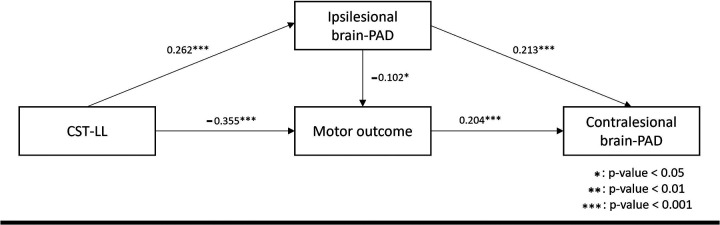
Findings: Larger total lesion size was positively associated with higher ipsilesional regional brain-PADs (older brain age) across most regions (p < 0.05), and with lower contralesional brain-PAD, notably in the ventral attention-language network (p < 0.05). Higher local lesion loads showed similar patterns. Specifically, lesion load in the salience network significantly influenced regional brain-PADs across both hemispheres. Machine learning models identified CST-LL, salience network lesion load, and regional brain-PAD in the contralesional frontoparietal network as the top three predictors of motor outcomes. Structural equation modeling revealed that larger stroke damage was associated with poorer motor outcomes (β = -0.355, p < 0.001), which were further linked to younger contralesional brain age (β = 0.204, p < 0.001), suggesting that severe motor impairment is linked to compensatory decreases in contralesional brain age.
Interpretation: Our findings reveal that larger stroke lesions are associated with accelerated aging in the ipsilesional hemisphere and paradoxically decelerated brain aging in the contralesional hemisphere, suggesting compensatory neural mechanisms. Assessing regional brain age may serve as a biomarker for neuroplasticity and inform targeted interventions to enhance motor recovery after stroke.
Fundings: Micheal J Fox Foundation, National Institutes of Health, Canadian Institutes of Health Research, National Health and Medical Research Council, Australian Brain Foundation, Wicking Trust, Collie Trust, and Sidney and Fiona Myer Family Foundation, National Heart Foundation, Hospital Israelita Albert Einstein, Australian Research Council Future Fellowship, Wellcome Trust, National Institute for Health Research Imperial Biomedical Research Centre, European Research Council, Deutsche Forschungsgemeinschaft, REACT Pilot, National Resource Center, Research Council of Norway, South-Eastern Norway Regional Health Authority, Norwegian Extra Foundation for Health and Rehabilitation, Sunnaas Rehabilitation Hospital HT, University of Oslo, and VA Rehabilitation Research and Development.
Keywords: graph convolutional network; lesion load; motor impairment; regional brain age; stroke outcome prediction; stroke recovery.
Conflict of interest statement
Competing Interests S. C. Cramer is a consultant for Constant Therapeutics, BrainQ, Myomo, MicroTransponder, Panaxium, Beren Therapeutics, Medtronic, Stream Biomedical, NeuroTrauma Sciences, and TRCare; C. A. Hanlon served as a consultant to MagStim, Roswell Park Cancer Insitute, and is an employee of BrainsWay; G. F. Wittenberg serves on the medical advisory boards for Myomo and NeuroInnovators; The other authors report no disclosures relevant to the manuscript.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous