

Rotator Cuff Injury: Pathogenesis, Biomechanics, and Repair
- PMID: 39574962
- PMCID: PMC11580759
- DOI: 10.26502/josm.511500167
Rotator Cuff Injury: Pathogenesis, Biomechanics, and Repair
Abstract
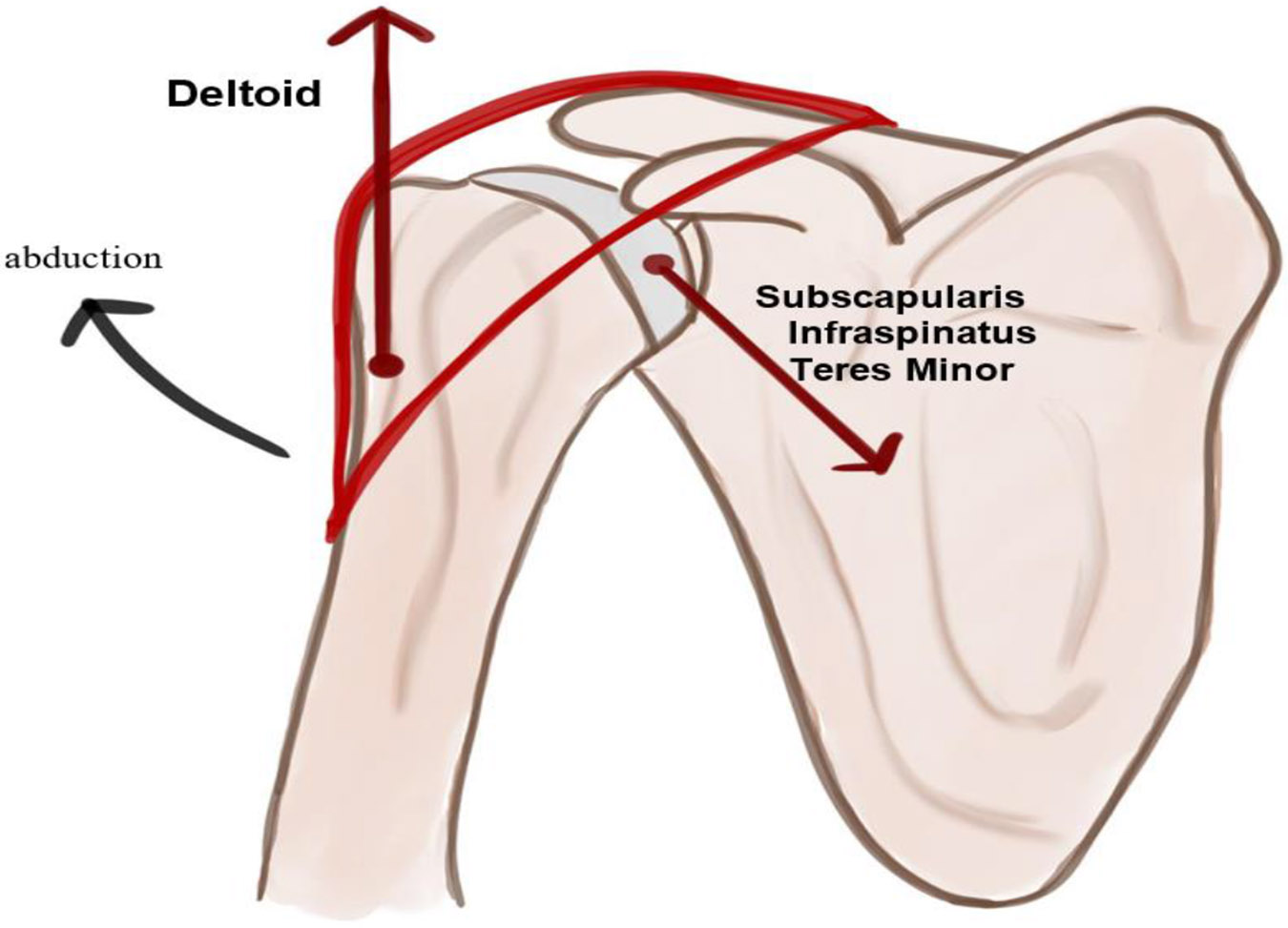
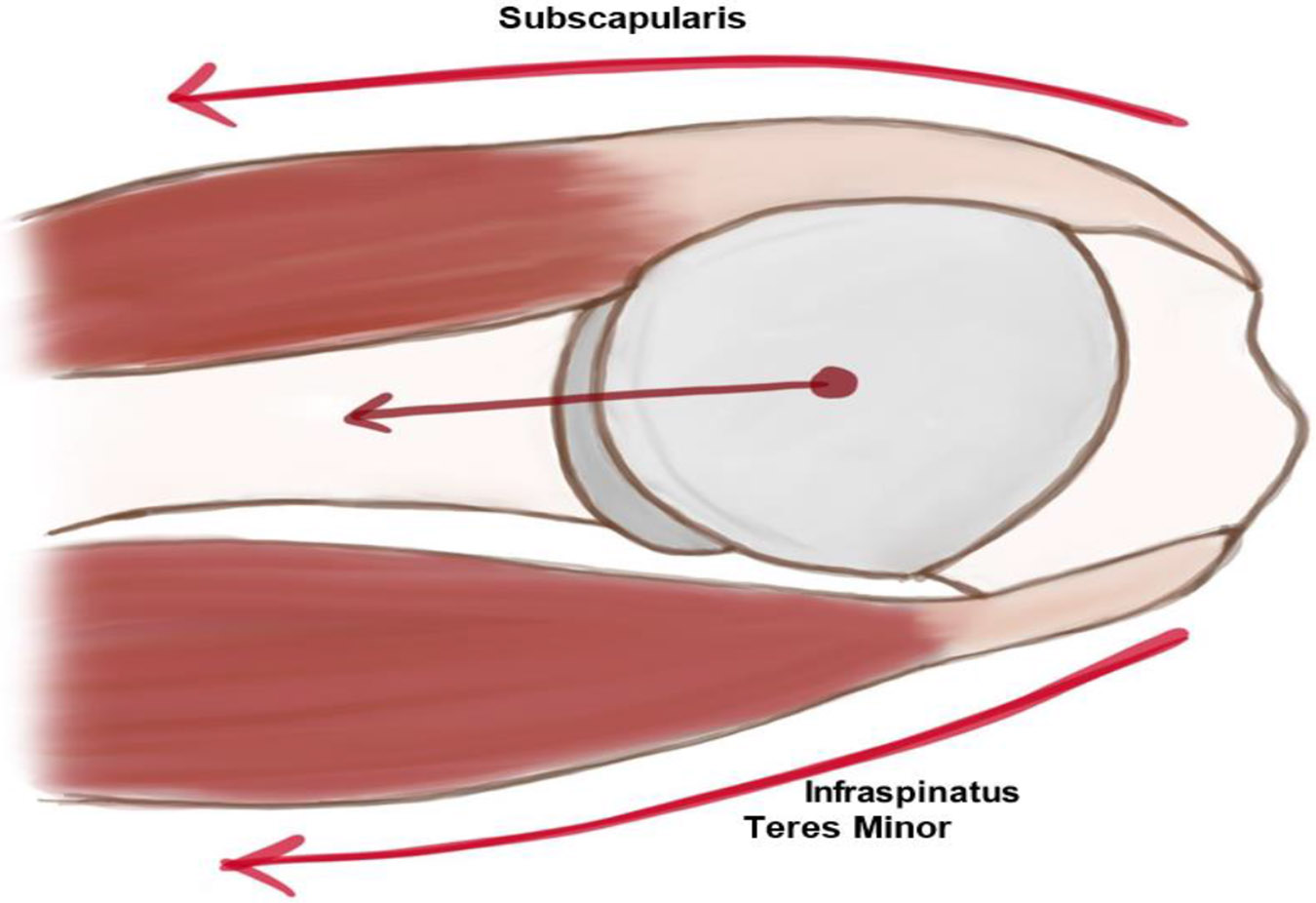
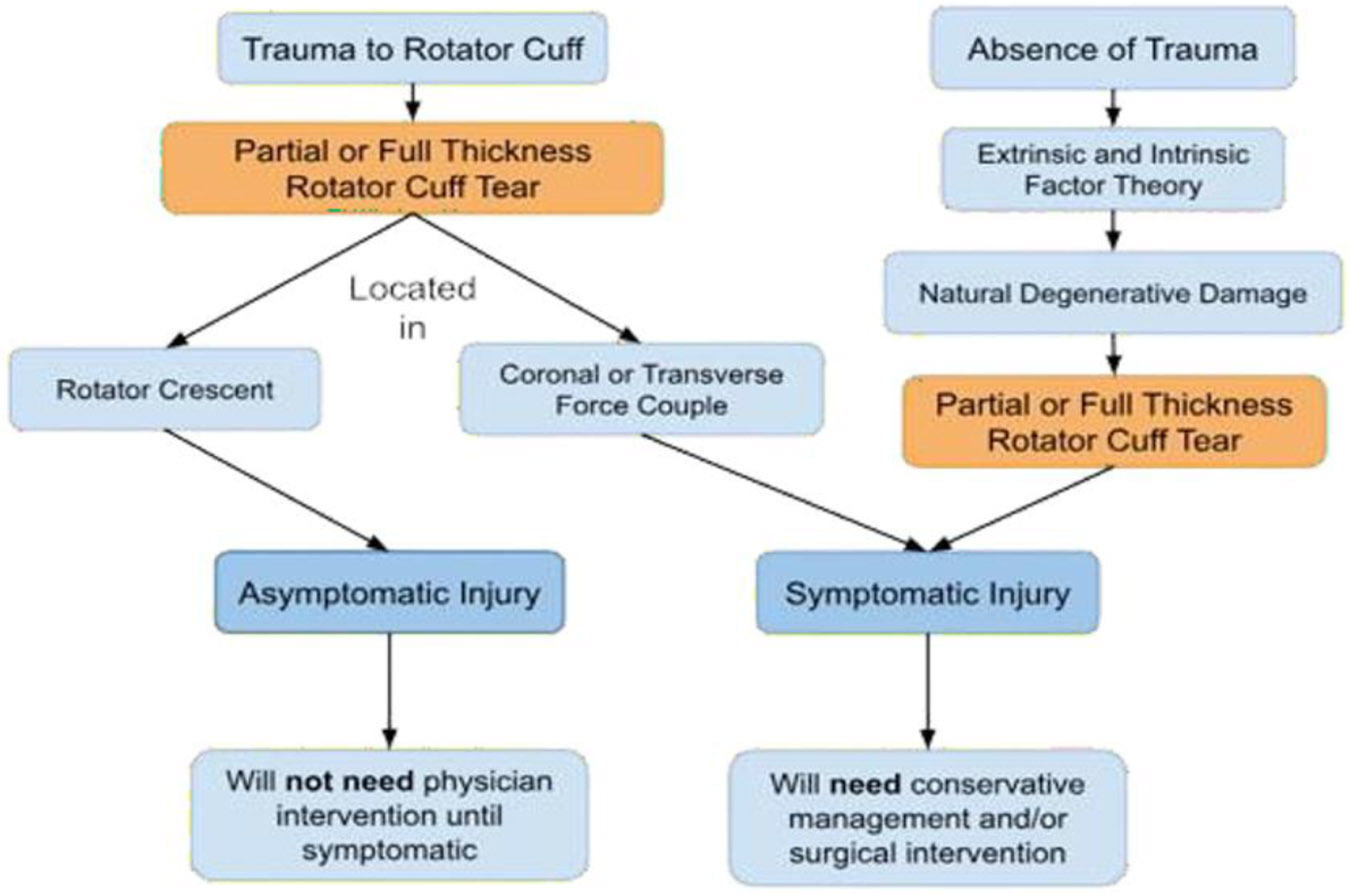
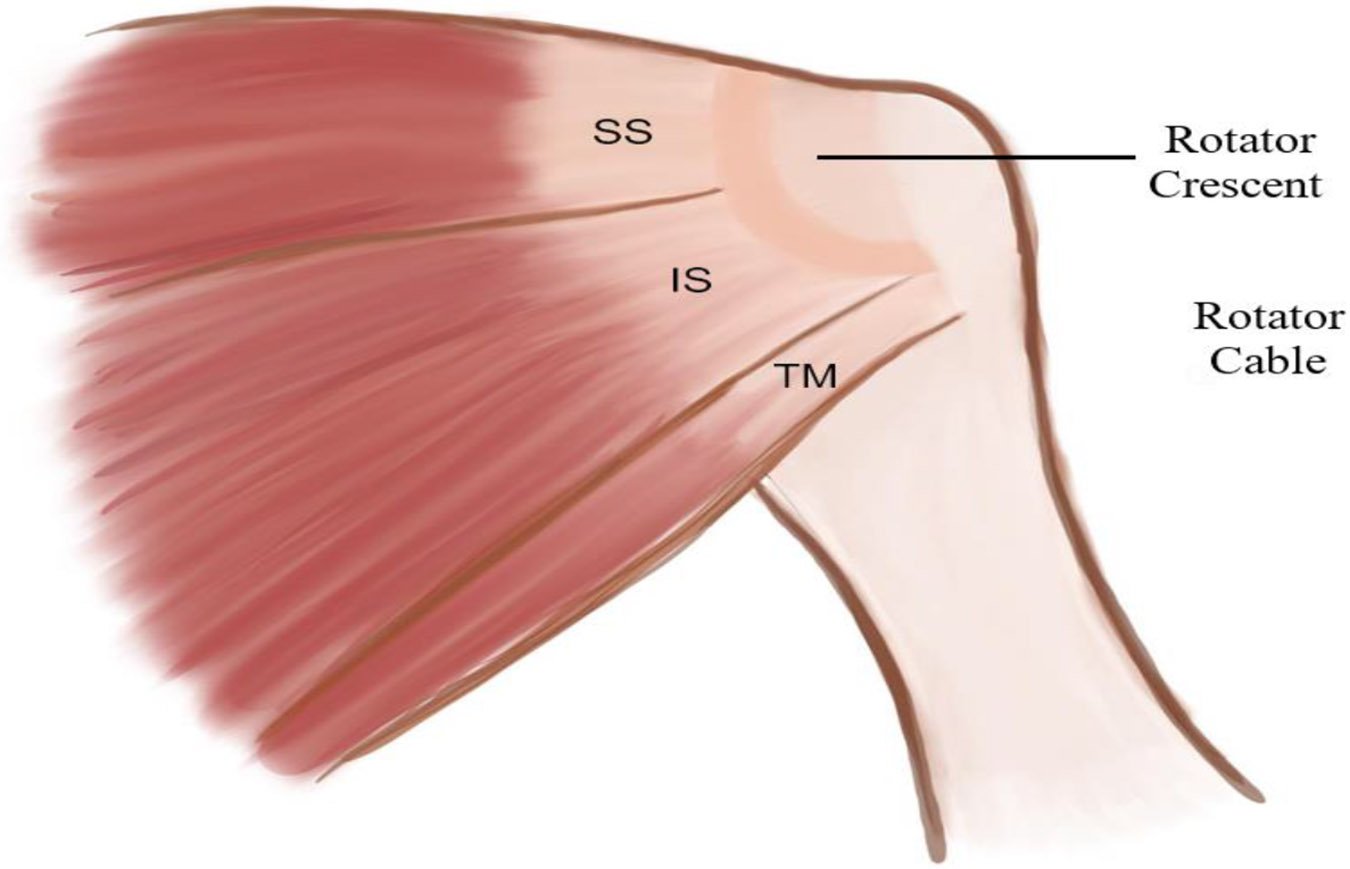
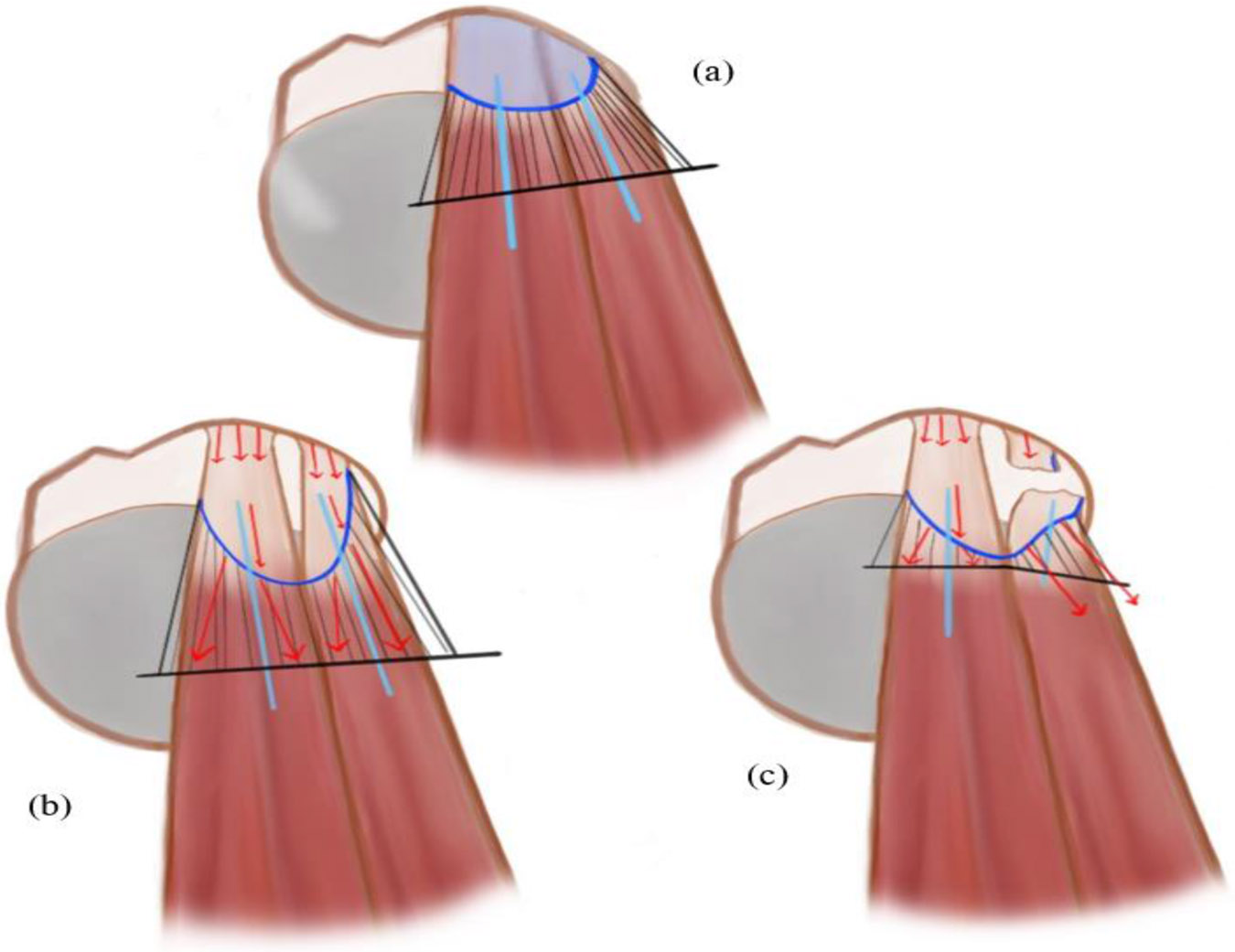
Anterior Rotator cuff tears are one of the most common surgically addressed disorders, as the tears in the tendon can affect anyone regardless of risk factors or activity level. The rotator cuff is responsible for most of the shoulder motion, hence the tendon-bone interface experiences immense stress making it incredibly prone to failure. Rotator cuff tendon tears can either occur due to trauma or natural degeneration of the rotator cuff. To help mitigate effects of high stress on the rotator cuff tendon-bone interface, the rotator cuff is intrinsically designed to redistribute stress through protective mechanisms, such as the rotator crescent or coronal-transverse force. But when the tear goes through the intrinsic protective mechanisms, the glenohumeral joint is left unstable and thus is no longer capable of its normal range of motion. Location, size, and type of rotator cuff tendon tears are the strongest indicators for interventional therapy. Surgical therapies demonstrate low success rates, as seen by the significantly high recurrence rate of rotator cuff reinjury following initial repair. This is due to extrinsically healing of rotator cuff tendons, instead of the more intrinsic healing, which causes rotator cuff tendons to not undergo the necessary biomechanical remodeling to prevent reinjury leading to a mechanically and functionally inferior healed tendon. In this article, we thoroughly discussed the underlying pathophysiology of rotator cuff tears from onset to repair to healing, demonstrating that rotator cuff tendon healing is an intrinsically flawed process, irrespective of the risk factors, occurrence of rotator cuff tears, or surgical treatment. Rotator cuff healing can only be successful if rotator cuff tendon repair surgery is augmented with biologics to promote a successful intrinsic healing environment.
Keywords: Biomechanics; Inflammation; Infraspinatus tendon; Rotator cuff injury; Rotator cuff repair; Supraspinatus tendon; Tendinopathy.
Conflict of interest statement
Competing interests: All authors have read the manuscript and declare no conflict of interest. No writing assistance was utilized in the production of this manuscript.
Figures
References
-
- Huegel J, Williams AA, Soslowsky LJ. Rotator cuff biology and biomechanics: a review of normal and pathological conditions. Curr Rheumatol Rep 17 (2015): 476. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources