

Succession of the multi-site microbiome along pancreatic ductal adenocarcinoma tumorigenesis
- PMID: 39575247
- PMCID: PMC11580624
- DOI: 10.3389/fimmu.2024.1487242
Succession of the multi-site microbiome along pancreatic ductal adenocarcinoma tumorigenesis
Abstract
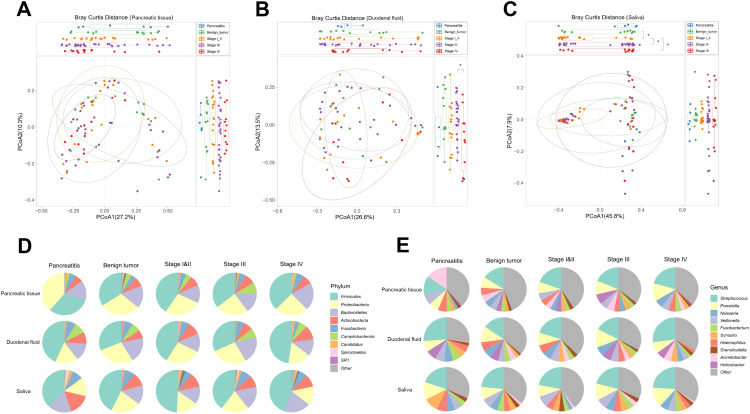
Background: To investigate microbial characteristics across multibody sites from chronic pancreatitis (CP), through pancreatic benign tumors, to pancreatic ductal adenocarcinoma (PDAC) at different stages.
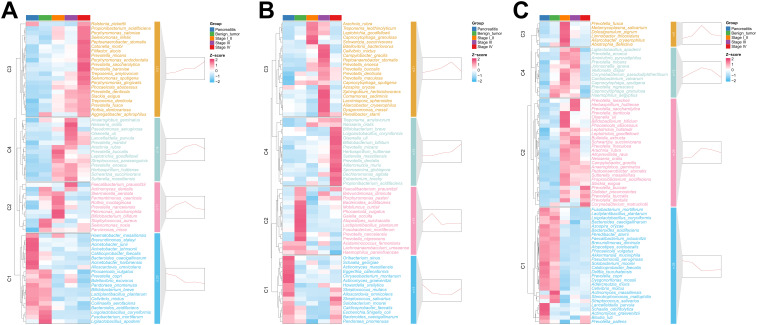
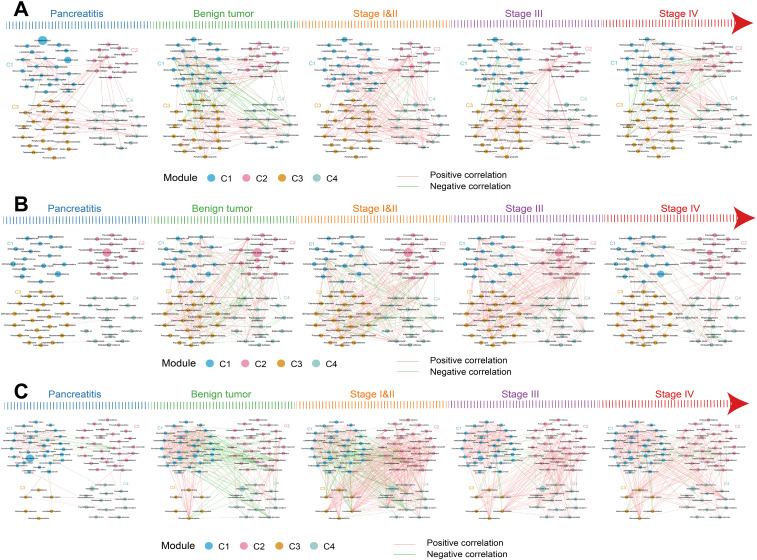
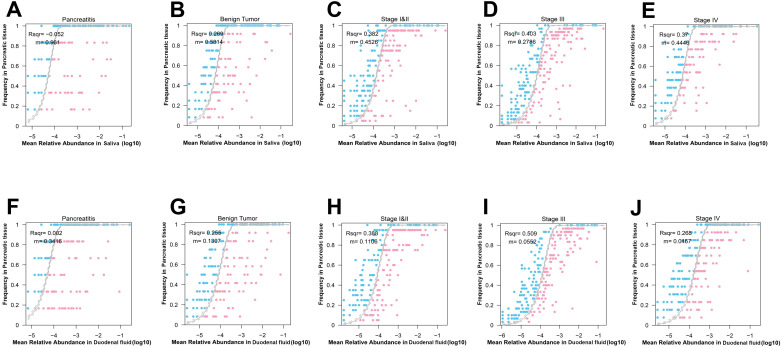
Methods: 16S ribosomal RNA (rRNA) amplicon sequencing was conducted on saliva, duodenal fluid, and pancreatic tissue obtained via endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) of patients with CP, pancreatic benign tumors, PDAC in stage I/II, III, and IV. The neutral community model (NCM) assessed the microbial assembly contribution and MaAslin2 identified the differential microbes.
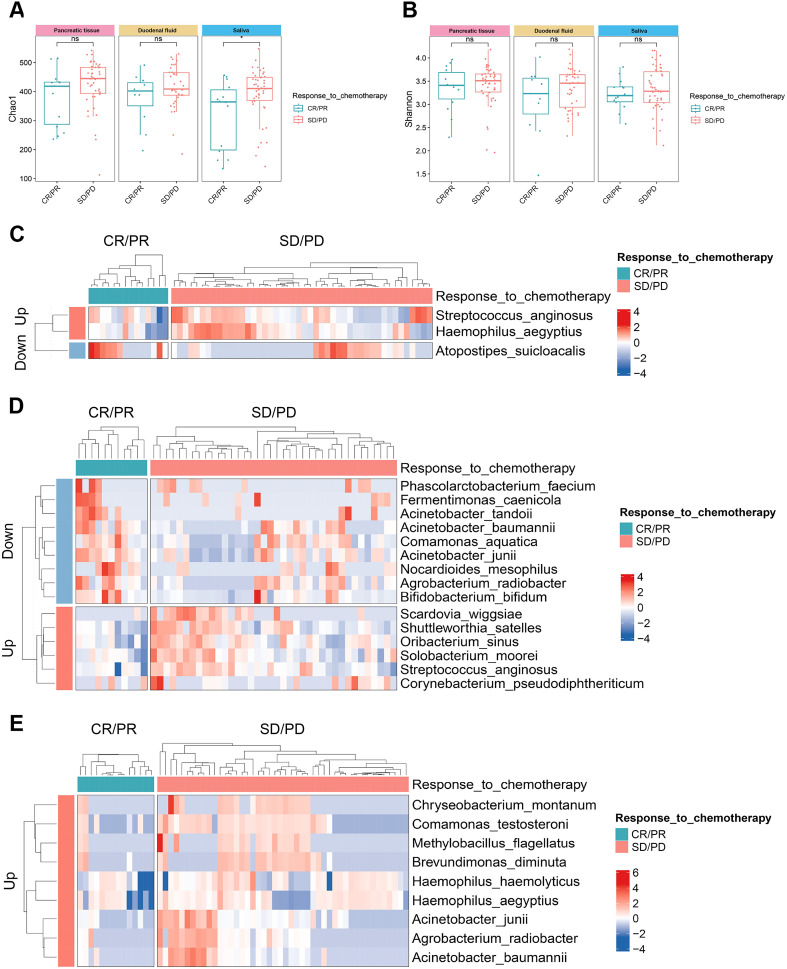
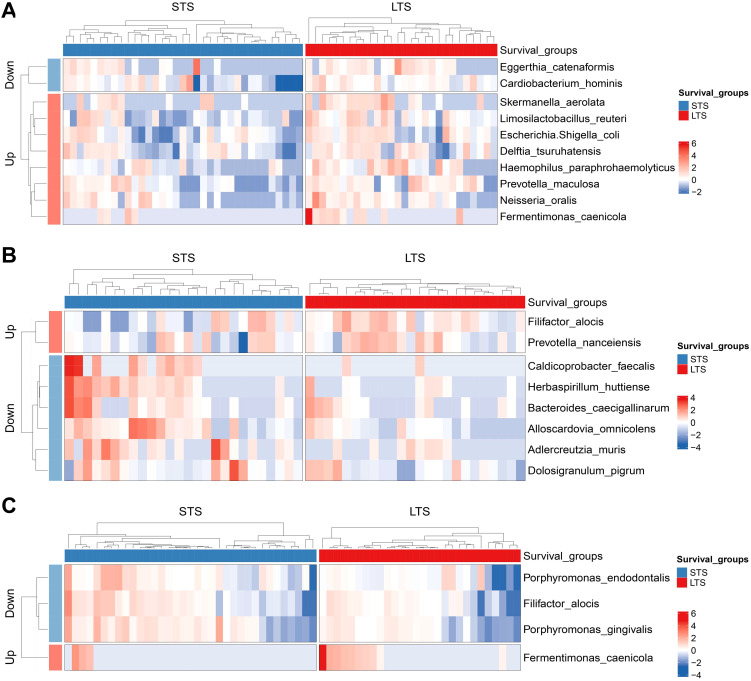
Results: From CP to stage IV PDAC patients, there was a marked surge in influence of salivary and duodenal microbiota on constitution of pancreatic microbial communities. Our observations revealed a successive alteration in microbial species across various bodily sites during PDAC tumorigenesis. Notably, Porphyromonas gingivalis, Treponema denticola, Peptoanaerobacter stomatis, Propionibacterium acidifaciens, Porphyromonas endodontalis, Filifactor alocis, etc., sequentially increased along PDAC progression in pancreatic tissue, whereas bacteria commonly used as probiotics Bifidobacterium breve, Lactiplantibacillus plantarum, etc., declined. Furthermore, the sequentially escalating trends of Peptoanaerobacter stomatis and Propionibacterium acidifaciens during PDAC tumorigenesis were mirrored in duodenal fluid and saliva. Porphyromonas gingivalis, Porphyromonas endodontalis, and Filifactor alocis, which intensified from CP to stage IV PDAC in pancreatic tissue, were also found to be enriched in saliva of patients with short-term survival (STS) compared with those with long-term survival (LTS).
Conclusions: Salivary and duodenal microorganisms were prominent factors in shaping pancreatic microbial landscape in PDAC context. Further exploration of these microbial entities is imperative to unravel their specific roles in PDAC pathogenesis, potentially yielding insights for future therapeutic strategies.
Keywords: endoscopic ultrasound-guided fine needle aspiration; microbiota; pancreatic neoplasms; pancreatitis; time series analysis.
Copyright © 2024 Zhu, Liang, Zhi, Li, Zhang, Chen, Wang, Wang, Zhong, Feng and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Microbiome and metabolome analysis in smoking and non-smoking pancreatic ductal adenocarcinoma patients.BMC Microbiol. 2024 Dec 27;24(1):541. doi: 10.1186/s12866-024-03688-5. BMC Microbiol. 2024. PMID: 39731043 Free PMC article.
-
Endoscopic ultrasound-guided fine-needle biopsy as a tool for studying the intra-tumoral microbiome in pancreatic ductal adenocarcinoma: a pilot study.Sci Rep. 2022 Jan 7;12(1):107. doi: 10.1038/s41598-021-04095-w. Sci Rep. 2022. PMID: 34997106 Free PMC article.
-
Integrated analysis of microbiome and metabolome reveals signatures in PDAC tumorigenesis and prognosis.Microbiol Spectr. 2024 Nov 5;12(11):e0096224. doi: 10.1128/spectrum.00962-24. Epub 2024 Oct 10. Microbiol Spectr. 2024. PMID: 39387592 Free PMC article.
-
Gut microbiome changes associated with chronic pancreatitis and pancreatic cancer: a systematic review and meta-analysis.Int J Surg. 2024 Sep 1;110(9):5781-5794. doi: 10.1097/JS9.0000000000001724. Int J Surg. 2024. PMID: 38847785 Free PMC article.
-
Applications of endoscopic ultrasound in pancreatic cancer.World J Gastroenterol. 2014 Jun 28;20(24):7808-18. doi: 10.3748/wjg.v20.i24.7808. World J Gastroenterol. 2014. PMID: 24976719 Free PMC article. Review.
Cited by
-
The dual role of gut microbiota in pancreatic cancer: new insights into onset and treatment.Ther Adv Med Oncol. 2025 Mar 15;17:17588359251324882. doi: 10.1177/17588359251324882. eCollection 2025. Ther Adv Med Oncol. 2025. PMID: 40093983 Free PMC article. Review.
-
Bacterial translocation signatures and subgingival microbiome in individuals with periodontitis.Clin Oral Investig. 2025 May 7;29(6):288. doi: 10.1007/s00784-025-06363-9. Clin Oral Investig. 2025. PMID: 40329006
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous