

Conformal proctectomy with sphincter preservation retains acceptable defecation functions in very low rectal cancer male patients
- PMID: 39575417
- PMCID: PMC11578961
- DOI: 10.3389/fonc.2024.1478467
Conformal proctectomy with sphincter preservation retains acceptable defecation functions in very low rectal cancer male patients
Abstract
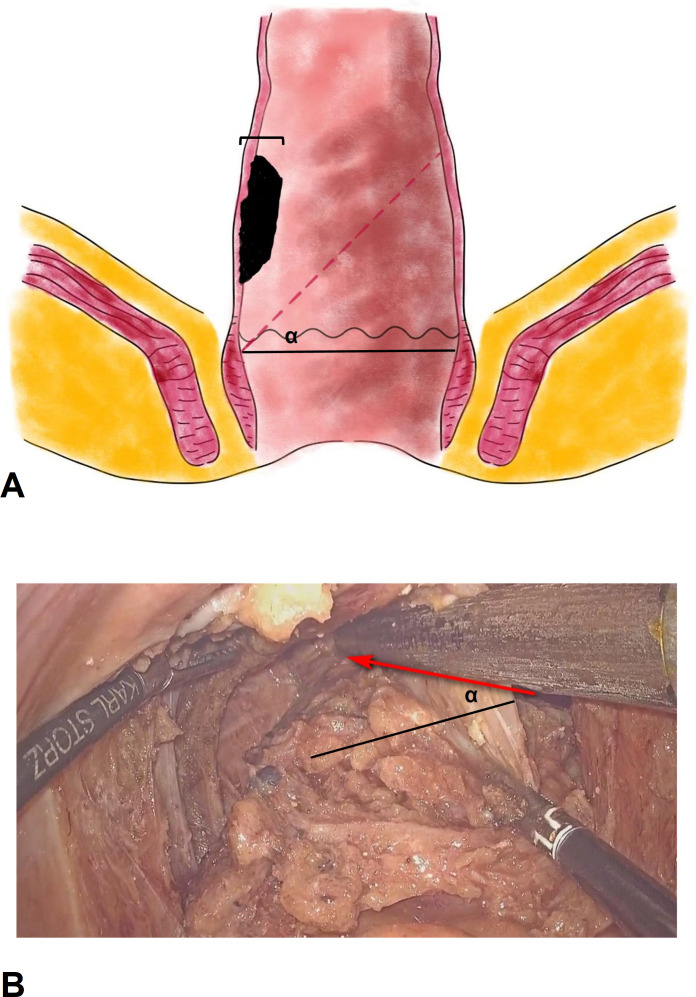
Background: Conformal proctectomy with sphincter preservation (CPSP) is designed to preserve the rectal wall as much as possible in very low rectal cancer patients. Evaluations of anal function and quality of life outcomes are lacking.
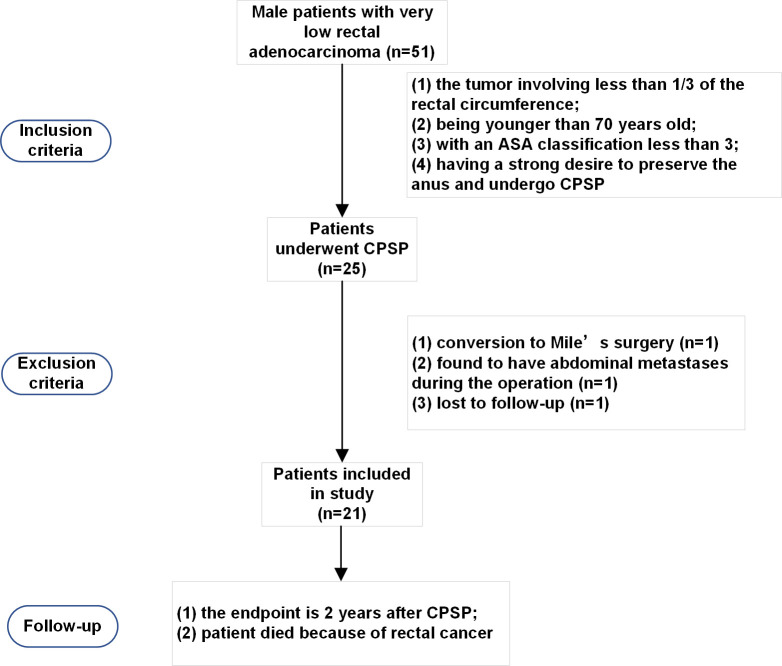
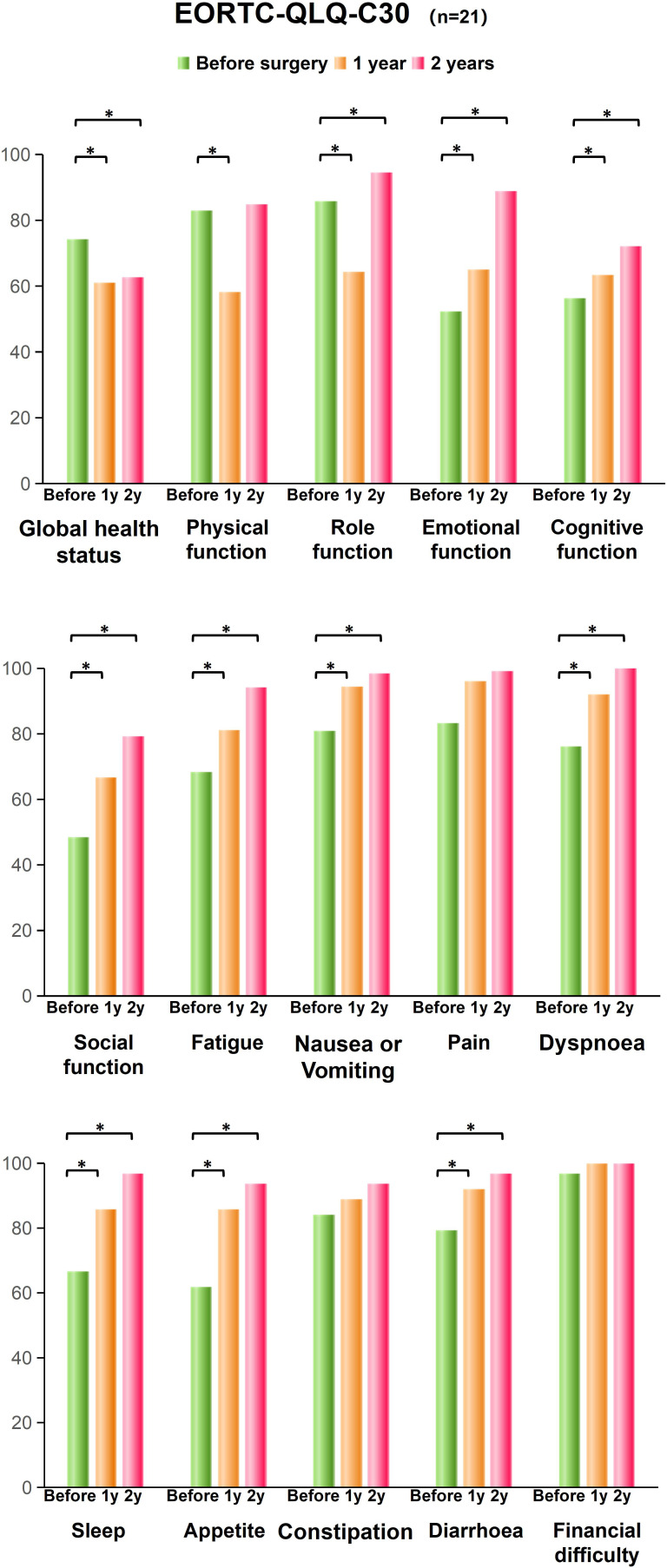
Methods: This study included male patients with very low (≤ 5 cm from the anal verge) rectal adenocarcinoma between January 1, 2020, and January 1, 2022. A LARS score questionnaire survey and EORTC-QLQ-CR38 questionnaire survey were administered.
Results: A total of 21 very low rectal cancer patients were enrolled in follow-up. The average age of the patients was 56.7 years, the tumors were 1.9 ± 0.6 cm in size, and the distance from the anal verge was 4.8 ± 0.5 cm. All patients were followed up, and the mean follow-up period was 2.7 ± 0.5 years. The LARS score increased significantly from 4.1 ± 2.8 before surgery to 19.1 ± 6.0 at the 1st year after surgery (P < 0.001) and then decreased to 13.1 ± 4.2 (P < 0.001) at the 2nd year. The quality of life of patients was also lower at the 1st year after surgery (61.1 ± 9.6 vs. 74.2 ± 11.2, P < 0.001) and was restored at the 2nd year after surgery (80.6 ± 11.9 vs. 74.2 ± 11.2, P = 0.029). During standard follow-up at the outpatient department, no rectal tumor relapse was confirmed in these patients, although 2 patients were found to have suspected recurrence of local lymph node metastasis.
Conclusions: These results suggest that the CPSP technique preserves acceptable defecation function and is a safe and feasible option for male patients with very low rectal cancer.
Clinical trial registration: https://www.chictr.org.cn/, identifier ChiCTR2100052094.
Keywords: anal function; clinical trial; quality of life; rectal cancer; total mesorectal excision.
Copyright © 2024 Chen, Zhang, Qiu, Zhou and Lin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Analysis on prognosis and influencing factors of postoperative low anterior resection syndrome for rectal cancer patients undergoing laparoscopic anus-preserving radical resection].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Jun 25;22(6):573-578. doi: 10.3760/cma.j.issn.1671-0274.2019.06.011. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 31238637 Chinese.
-
Comparison of anal function and quality of life after conformal sphincter preservation operation and intersphincteric resection of very low rectal cancer: a multicenter, retrospective, case-control analysis.Tech Coloproctol. 2023 Dec;27(12):1275-1287. doi: 10.1007/s10151-023-02819-w. Epub 2023 May 29. Tech Coloproctol. 2023. PMID: 37248369 Free PMC article.
-
[Quality of life of patients with locally advanced rectal cancer after neoadjuvant therapy and sphincter-preserving surgery].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 Apr 25;25(4):348-356. doi: 10.3760/cma.j.cn441530-20210808-00315. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 35461204 Chinese.
-
[Risk factor analysis of low anterior resection syndrome after anal sphincter preserving surgery for rectal carcinoma].Zhonghua Wei Chang Wai Ke Za Zhi. 2017 Mar 25;20(3):289-294. Zhonghua Wei Chang Wai Ke Za Zhi. 2017. PMID: 28338162 Chinese.
-
[Analysis on the technical characteristics and clinical efficacy of robotic-assisted intersphincteric resection for patients with low rectal cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Dec 25;22(12):1137-1143. doi: 10.3760/cma.j.issn.1671-0274.2019.12.008. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 31874529 Chinese.
Cited by
-
The Review of Modified Intersphincteric Resection in the Treatment of Ultra-Low Rectal Cancer.Curr Treat Options Oncol. 2025 Feb;26(2):84-91. doi: 10.1007/s11864-025-01291-y. Epub 2025 Jan 23. Curr Treat Options Oncol. 2025. PMID: 39847237 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources