

Drug-Coated Balloons Versus Drug-Eluting Stents or Plain Old Balloon Angioplasty: A Long-Term in-Stent Restenosis Study
- PMID: 39575722
- PMCID: PMC11681599
- DOI: 10.1161/JAHA.124.036839
Drug-Coated Balloons Versus Drug-Eluting Stents or Plain Old Balloon Angioplasty: A Long-Term in-Stent Restenosis Study
Abstract
Background: Balloon angioplasty with drug-coated balloons (DCBs) is frequently used during percutaneous coronary intervention for in-stent restenosis. Despite its frequent use, there is a lack of long-term data on the efficacy of DCB angioplasty. We conducted an investigation on the long-term efficacy outcome of in-stent restenosis, comparing DCBs, drug-eluting stents, and plain old balloon angioplasty.
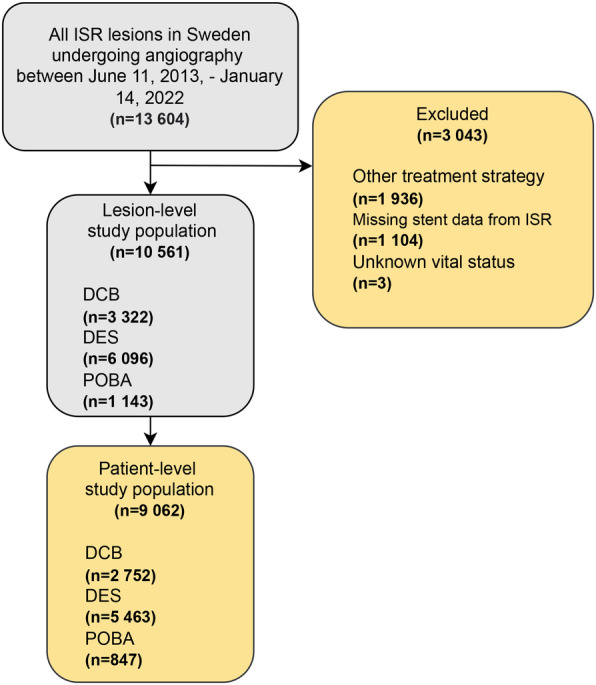
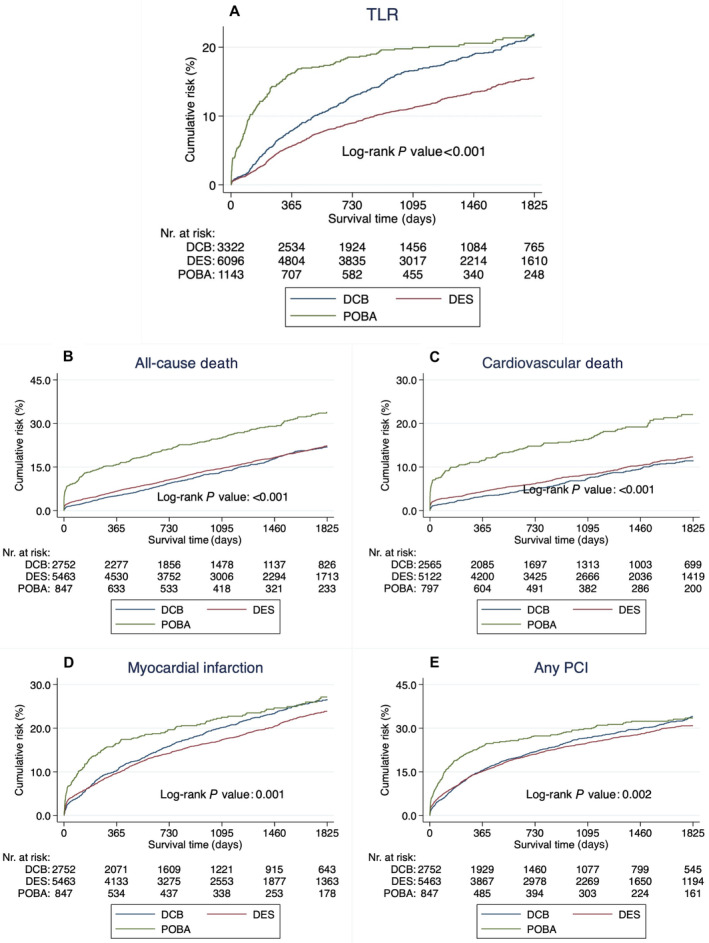
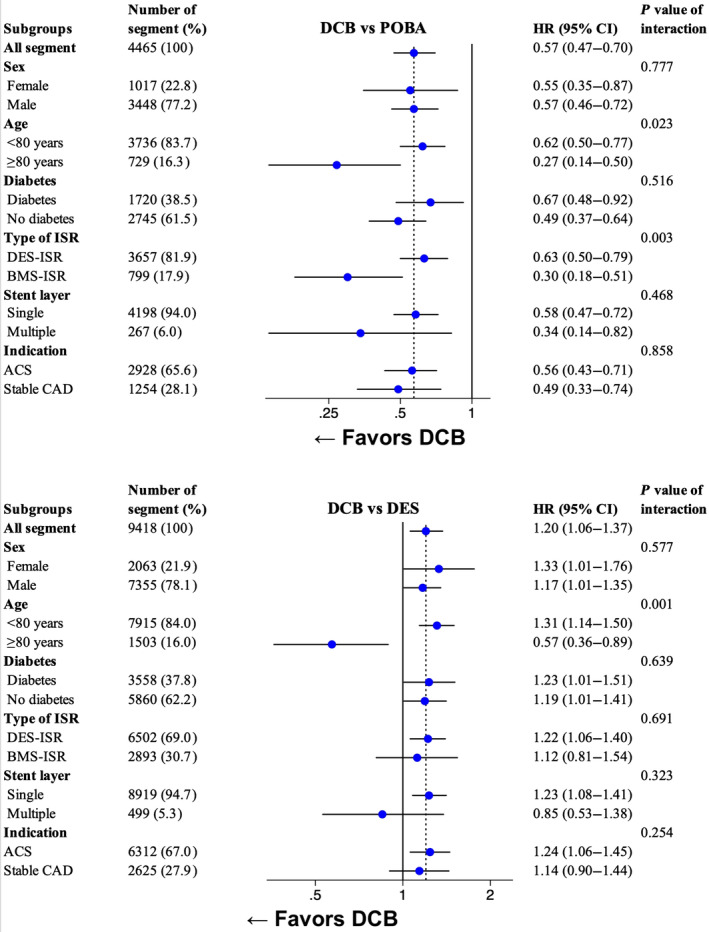
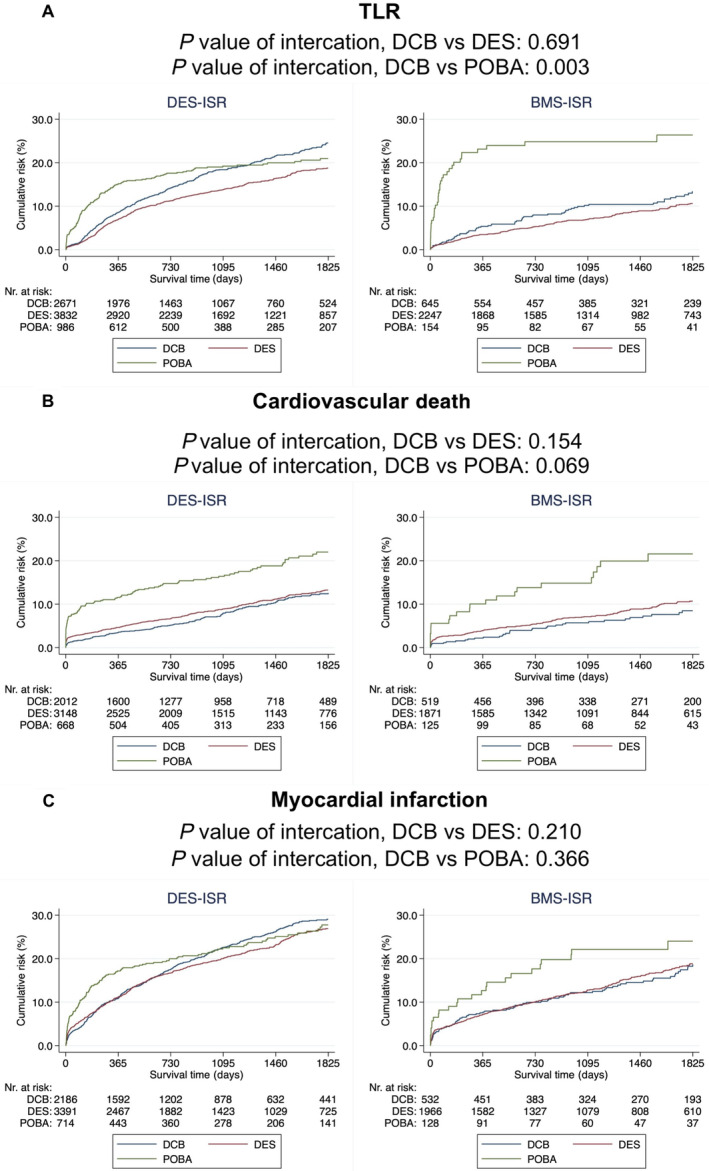
Methods and results: We conducted a nationwide analysis from the SCAAR (Swedish Coronary Angiography and Angioplasty Registry) including in-stent restenosis lesions undergoing coronary angiography between June 11, 2013, and January 14, 2022. The primary outcome of this study was target-lesion revascularization within a 5-year follow-up. Secondary outcomes included all-cause death, cardiovascular death, myocardial infarction, and any percutaneous coronary intervention. The outcomes were analyzed using a multivariable Cox proportional hazard model or Poisson regression, as appropriate. A total of 10 561 lesions from 9062 patients were included. Compared with plain old balloon angioplasty, the use of DCB angioplasty was associated with less target-lesion revascularization (risk ratio, 0.69 [95% CI, 0.57-0.82]), all-cause death (risk ratio, 0.72 [95% CI, 0.59-0.88]), and cardiovascular death (hazard ratio [HR], 0.59 [95% CI, 0.45-0.78]). No difference was observed for myocardial infarction or any percutaneous coronary intervention. Compared with drug-eluting stents, the use of DCBs was associated with higher rates of target-lesion revascularization (HR, 1.20 [95% CI, 1.06-1.37]). No difference was observed for all-cause death, cardiovascular death, myocardial infarction, or any percutaneous coronary intervention.
Conclusions: In this long-term nationwide analysis, the use of DCB angioplasty showed superior outcomes compared with plain old balloon angioplasty within 5 years but higher rates of repeat revascularizations compared with drug-eluting stents.
Keywords: drug‐coated balloon; drug‐eluting stent; in‐stent restenosis; plain old balloon angioplasty; target‐lesion revascularization.
Figures
Comment in
-
Drug-Coated Balloons in In-Stent Restenosis, a New Standard of Care or Yesterday's News?J Am Heart Assoc. 2024 Dec 3;13(23):e038508. doi: 10.1161/JAHA.124.038508. Epub 2024 Nov 26. J Am Heart Assoc. 2024. PMID: 39588665 Free PMC article. No abstract available.
References
-
- Grines CL, Cox DA, Stone GW, Garcia E, Mattos LA, Giambartolomei A, Brodie BR, Madonna O, Eijgelshoven M, Lansky AJ, et al. Coronary angioplasty with or without stent implantation for acute myocardial infarction. Stent primary angioplasty in myocardial infarction study group. N Engl J Med. 1999;341:1949–1956. doi: 10.1056/NEJM199912233412601 - DOI - PubMed
-
- Morice MC, Serruys PW, Sousa JE, Fajadet J, Ban Hayashi E, Perin M, Colombo A, Schuler G, Barragan P, Guagliumi G, et al. Randomized study with the sirolimus‐coated bx velocity balloon‐expandable stent in the treatment of patients with de novo native coronary artery lesions. A randomized comparison of a sirolimus‐eluting stent with a standard stent for coronary revascularization. N Engl J Med. 2002;346:1773–1780. doi: 10.1056/NEJMoa012843 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
