

Hypotension after unilateral versus bilateral spinal anaesthesia: A Systematic review with meta-analysis
- PMID: 39575900
- PMCID: PMC11784910
- DOI: 10.1097/EJA.0000000000002098
Hypotension after unilateral versus bilateral spinal anaesthesia: A Systematic review with meta-analysis
Abstract
Background: Spinal anaesthesia is frequently used in surgical procedures involving the lower abdomen and extremities, however, the occurrence of hypotension remains a common and clinically important adverse effect. Unilateral spinal anaesthesia seems to be a promising approach to minimise this complication but the effectiveness of this remains controversial.
Objective: A meta-analysis was undertaken to evaluate the superiority of unilateral spinal anaesthesia over bilateral spinal anaesthesia with regard to the incidence of hypotension and other complications.
Design: Systematic reviews and meta-analysis of randomised controlled trials (RCTs).
Date sources: PUBMED, Embase, Web of Science and Cochrane Central Register of Controlled Trials databases were searched from their inception to 5 March 2024.
Eligibility criteria: Randomised controlled trials (RCTs) comparing unilateral spinal anaesthesia with bilateral spinal anaesthesia were eligible for inclusion. Observational studies, case reports, case series, and studies not conducted in humans were excluded. The incidence of hypotension, vasopressor requirement, and other complications were compared. Heterogeneity was assessed by subgroup analyses and sensitivity analysis.
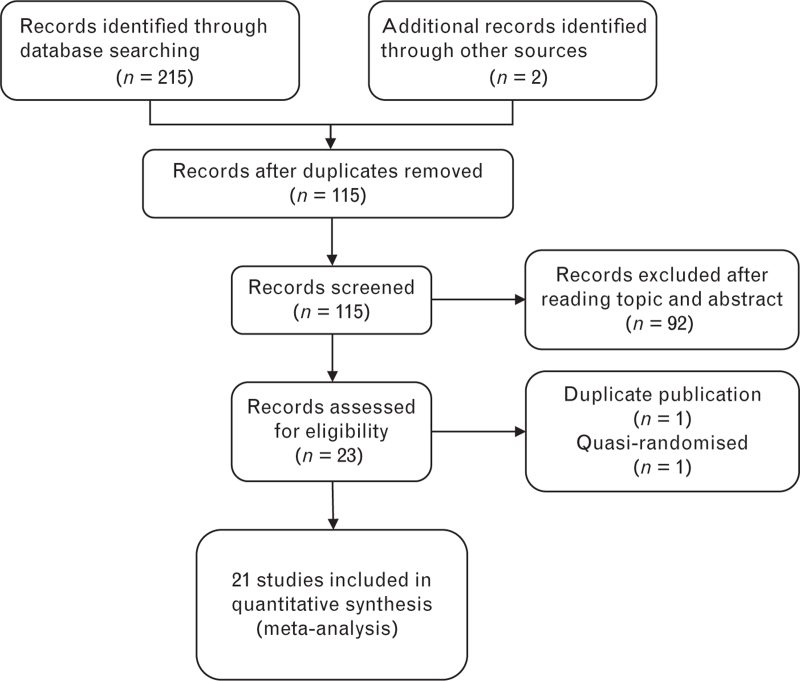
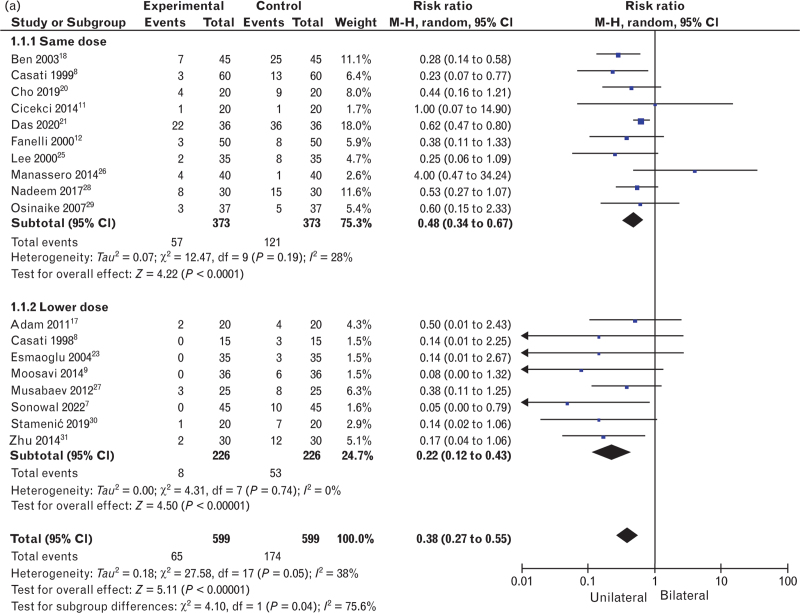
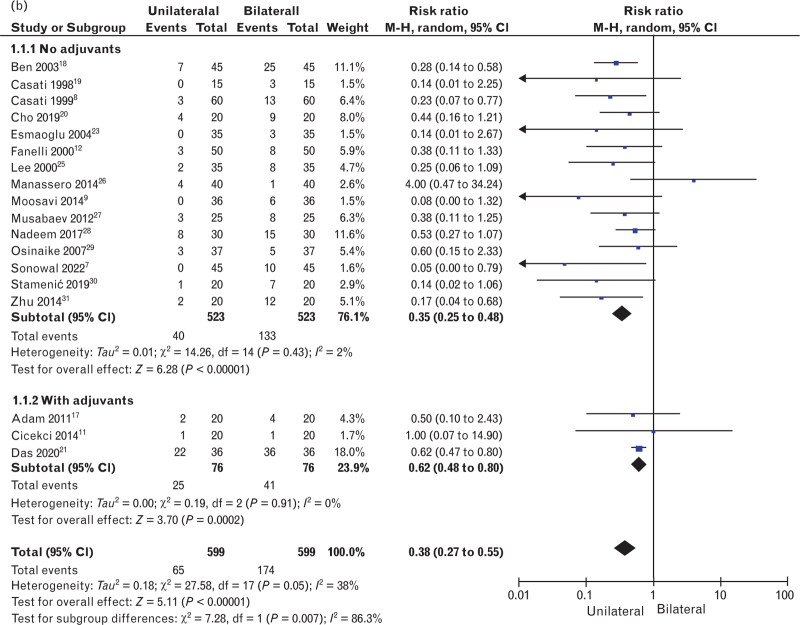
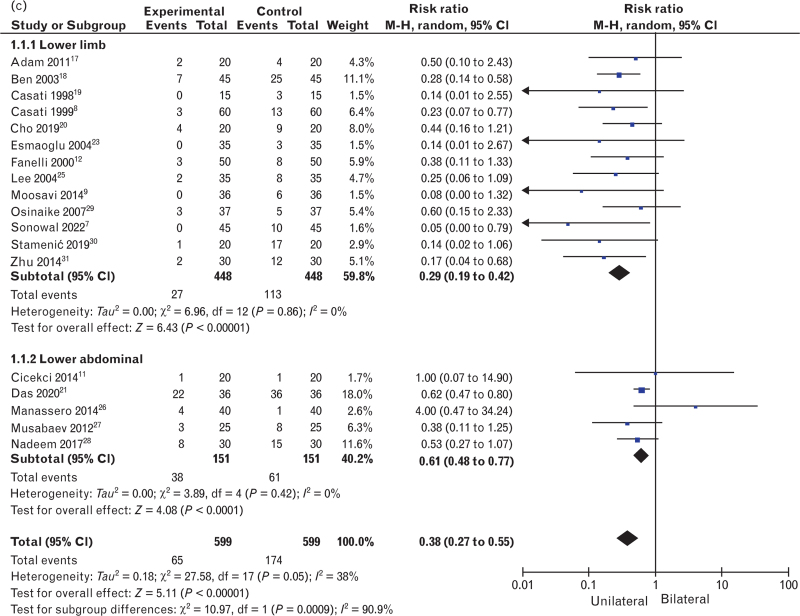
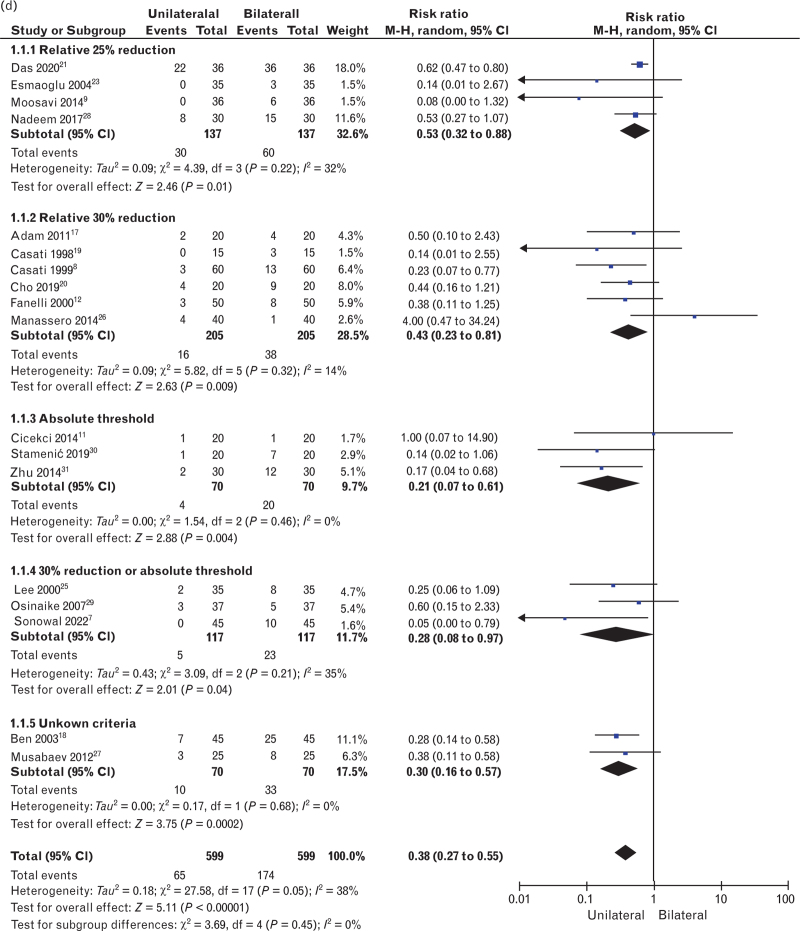
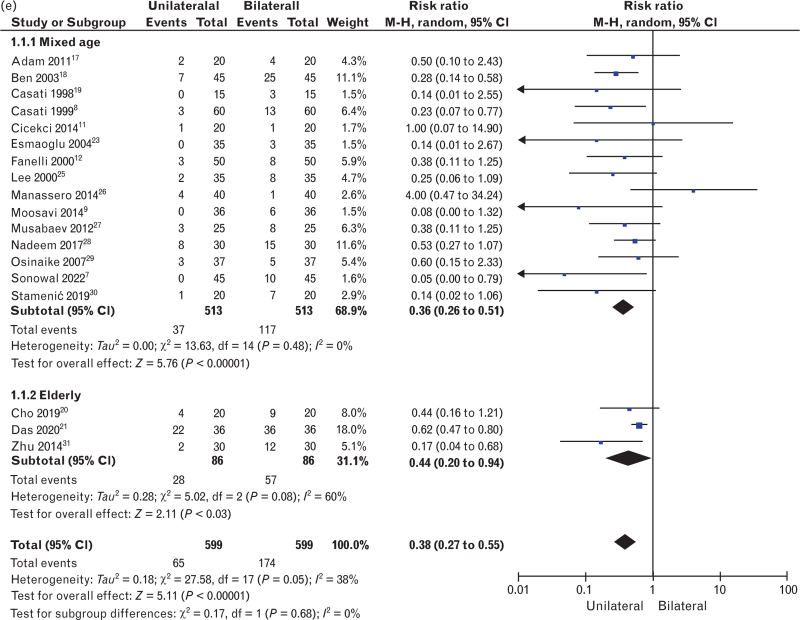
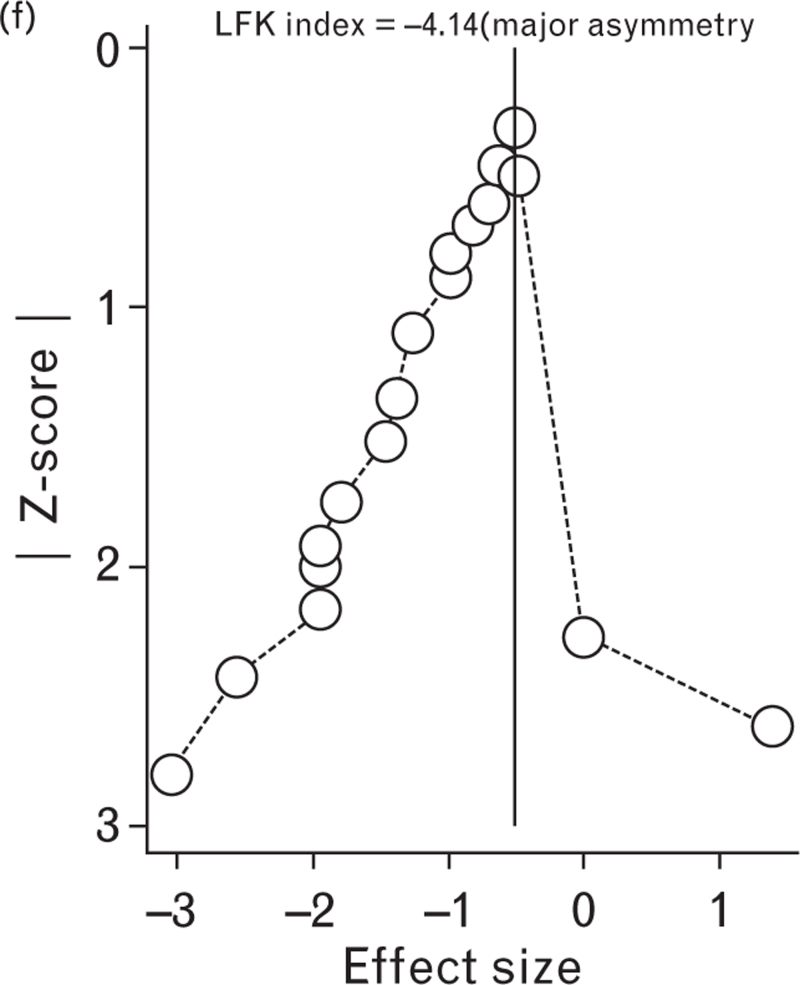
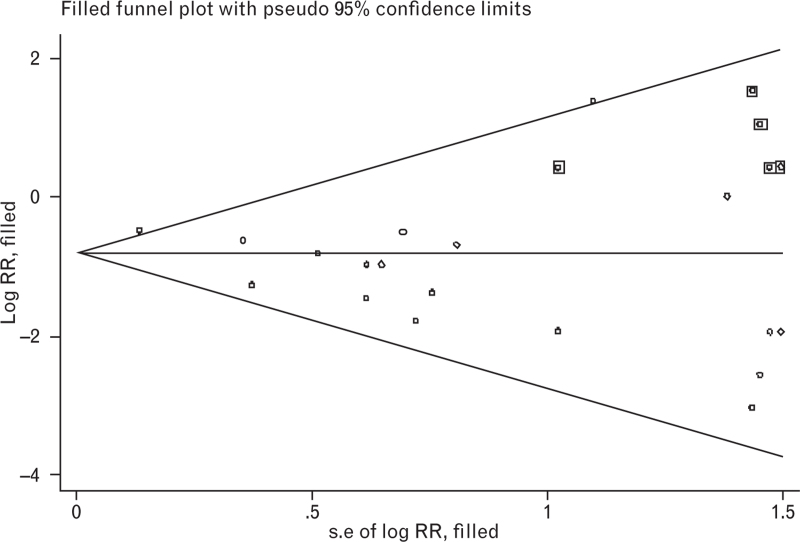
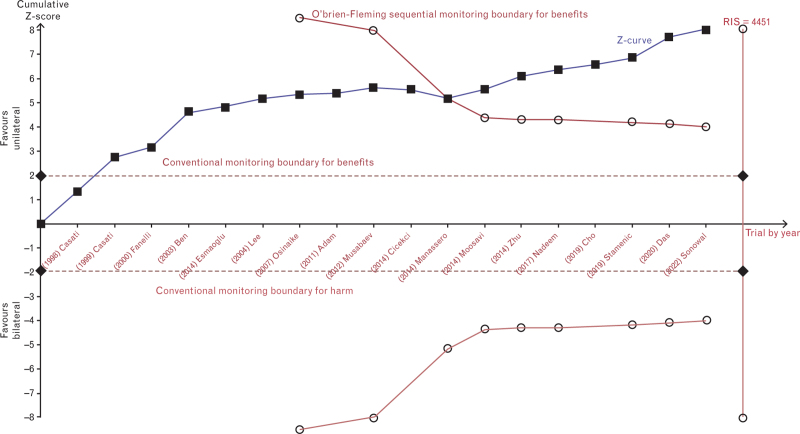
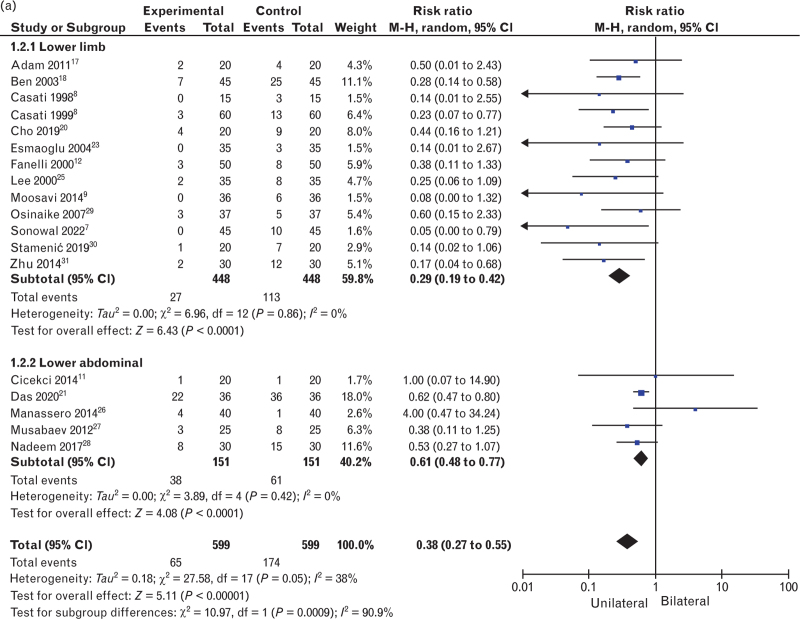
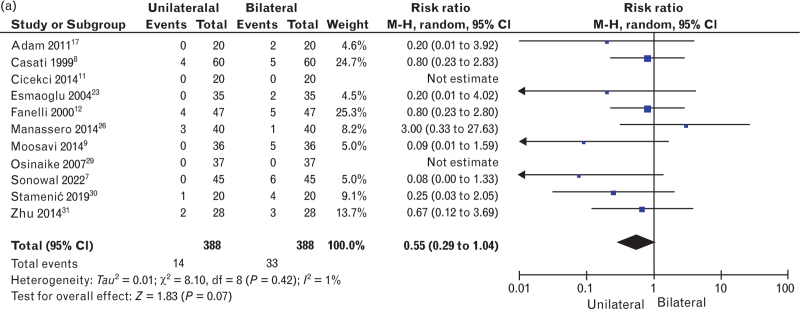
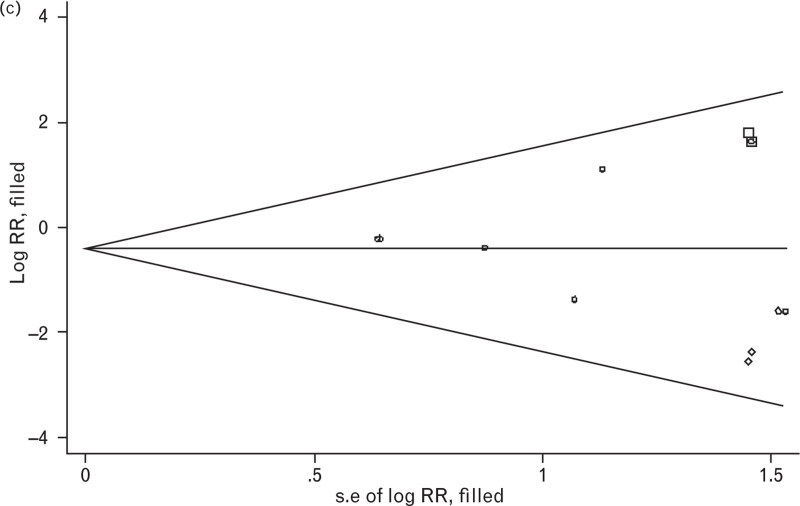
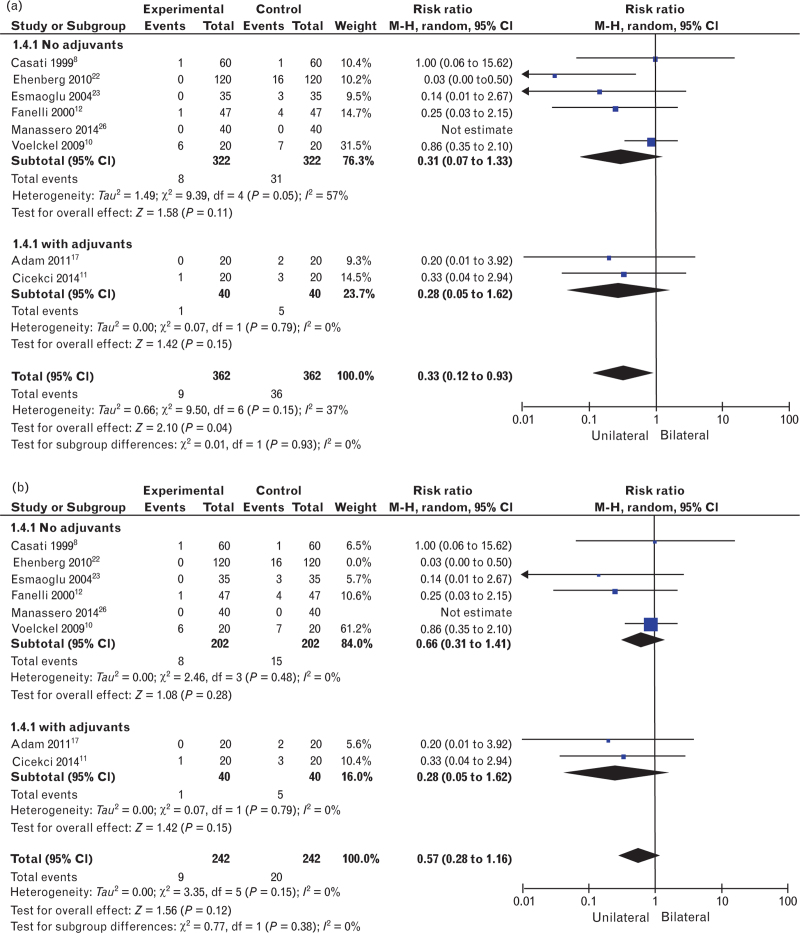
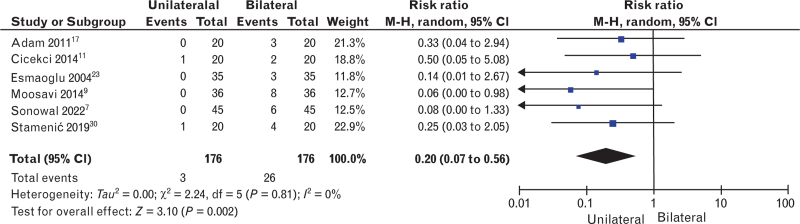
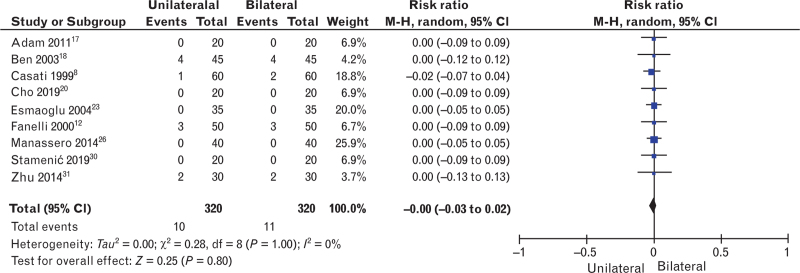
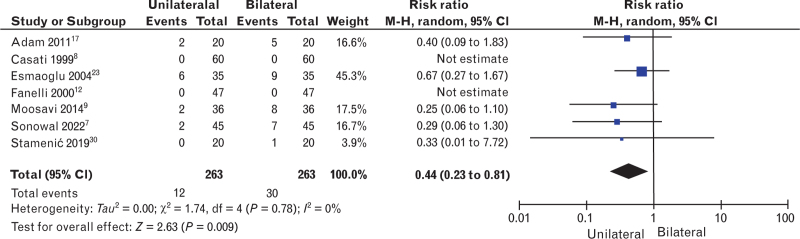
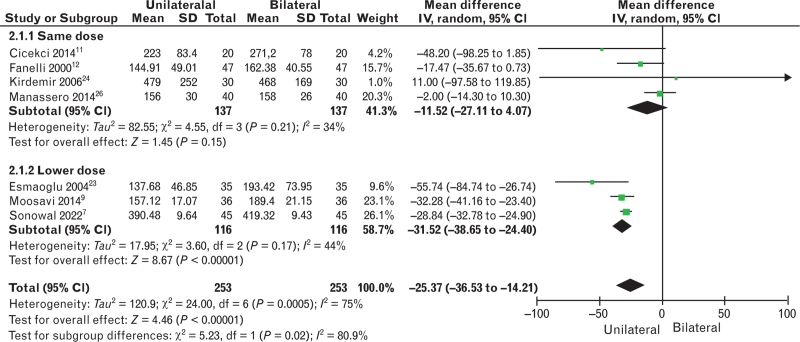
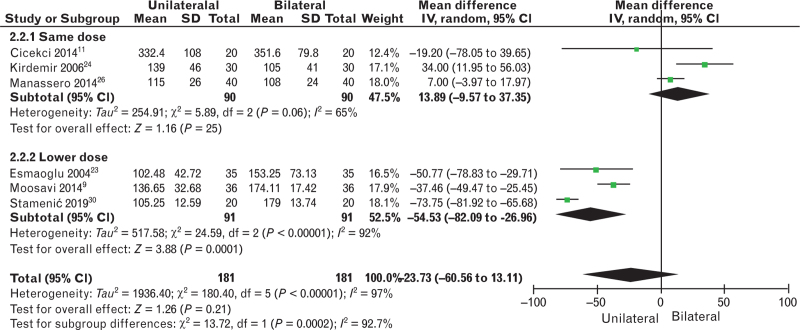
Results: Twenty-one trials involving 1358 patients undergoing unilateral lower extremity surgery or lower abdominal surgery were included in the meta-analysis. Hyperbaric solutions were used in most trials. The Mantel-Haenszel random-effect model was used for the analysis of binary endpoints, reported as relative risk (RR) with a 95% confidence interval (CI). The incidence of hypotension was significantly lower in the unilateral spinal anaesthesia group compared with the bilateral spinal anaesthesia (RR 0.38, 95% CI 0.27 to 0.55; P < 0.001; I2 = 38%). Subgroup analysis shows that the occurrence of hypotension was significantly lower in the unilateral subgroup, regardless of dosage, surgical site, adjuvants to the local anaesthetics, and different definitions of hypotension.
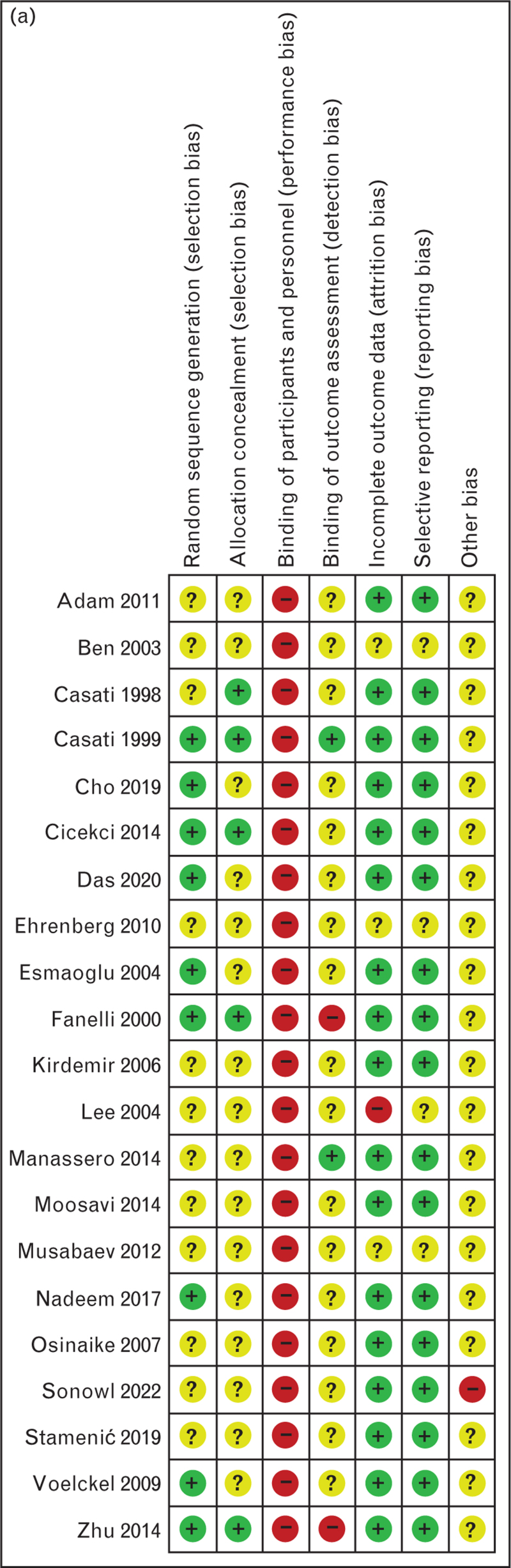
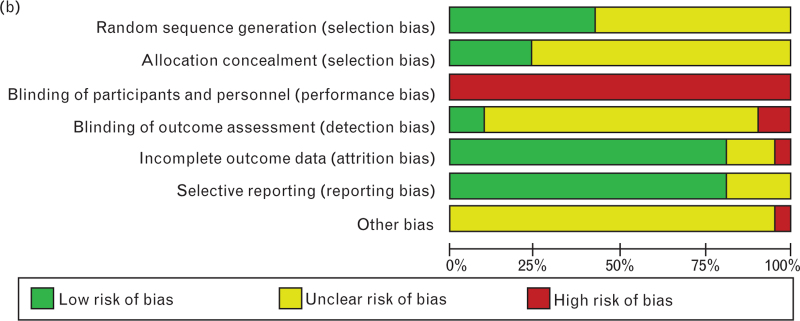
Conclusions: Unilateral spinal anaesthesia is associated with a significant reduction in the occurrence of hypotension, despite variations in the definition of hypotension, adjuvants, and site of surgery. These results favour the use of lateral spinal anaesthesia in patients undergoing unilateral lower abdominal or lower limb surgery. However, the GRADE assessment of the quality of evidence was 'low' due to the high risk of bias and heterogeneity. All the results should be treated with caution.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Society of Anaesthesiology and Intensive Care.
Figures

Similar articles
-
Techniques for preventing hypotension during spinal anaesthesia for caesarean section.Cochrane Database Syst Rev. 2020 Jul 1;7(7):CD002251. doi: 10.1002/14651858.CD002251.pub4. Cochrane Database Syst Rev. 2020. PMID: 32619039 Free PMC article.
-
Transient neurological symptoms (TNS) following spinal anaesthesia with lidocaine versus other local anaesthetics in adult surgical patients: a network meta-analysis.Cochrane Database Syst Rev. 2019 Dec 1;12(12):CD003006. doi: 10.1002/14651858.CD003006.pub4. Cochrane Database Syst Rev. 2019. PMID: 31786810 Free PMC article.
-
Predictive ability of pulse oximetry-derived indices for hypotension after spinal anaesthesia for caesarean section: protocol for a systematic review and meta-analysis.BMJ Open. 2023 Jun 23;13(6):e069309. doi: 10.1136/bmjopen-2022-069309. BMJ Open. 2023. PMID: 37355260 Free PMC article.
-
Paravertebral anaesthesia with or without sedation versus general anaesthesia for women undergoing breast cancer surgery.Cochrane Database Syst Rev. 2021 Feb 25;2(2):CD012968. doi: 10.1002/14651858.CD012968.pub2. Cochrane Database Syst Rev. 2021. PMID: 33629404 Free PMC article.
-
Leg Compression Versus Control for Prevention of Spinal Anesthesia Induced Hypotension in Elective Cesarean Delivery: A Meta-Analysis of Randomized Controlled Trials.J Perianesth Nurs. 2022 Aug;37(4):501-508. doi: 10.1016/j.jopan.2021.10.011. Epub 2022 Mar 4. J Perianesth Nurs. 2022. PMID: 35256251 Review.
Cited by
-
ED50 and ED95 of hypobaric ropivacaine during unilateral spinal anesthesia in older patients undergoing hip replacement surgery.Front Med (Lausanne). 2025 Jul 24;12:1571574. doi: 10.3389/fmed.2025.1571574. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40776928 Free PMC article.
-
Perfusion index as a predictor of hypotension after spinal anesthesia in lower extremity orthopedic surgery: a prospective observational trial.BMC Surg. 2025 Aug 7;25(1):348. doi: 10.1186/s12893-025-03036-y. BMC Surg. 2025. PMID: 40770325 Free PMC article.
References
-
- Carpenter RL, Caplan RA, Brown DL, et al. . Incidence and risk factors for side effects of spinal anesthesia. Anesthesiology 1992; 76:906–916. - PubMed
-
- Ferré F, Marty P, Bruneteau L, et al. . Prophylactic phenylephrine infusion for the prevention of hypotension after spinal anesthesia in the elderly: a randomized controlled clinical trial. J Clin Anesth 2016; 35:99–106. - PubMed
-
- Walsh M, Devereaux PJ, Garg AX, et al. . Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery: toward an empirical definition of hypotension. Anesthesiology 2013; 119:507–515. - PubMed
-
- Lee JE, George RB, Habib AS. Spinal-induced hypotension: incidence, mechanisms, prophylaxis, and management: summarizing 20 years of research. Best Pract Res Clin Anaesthesiol 2017; 31:57–68. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
