

Efanesoctocog Alfa Versus Emicizumab in Adolescent and Adult Patients With Haemophilia A Without Inhibitors
- PMID: 39576432
- PMCID: PMC11782328
- DOI: 10.1007/s12325-024-03031-4
Efanesoctocog Alfa Versus Emicizumab in Adolescent and Adult Patients With Haemophilia A Without Inhibitors
Abstract
Introduction: The phase 3 XTEND-1 trial (NCT04161495) demonstrated that efanesoctocog alfa prophylaxis provided superior bleed protection compared with pre-trial factor VIII (FVIII) prophylaxis in patients with severe haemophilia A. The aim of this study was to indirectly compare the efficacy of efanesoctocog alfa with non-factor replacement therapy emicizumab in adolescent and adult patients with severe haemophilia A without inhibitors.
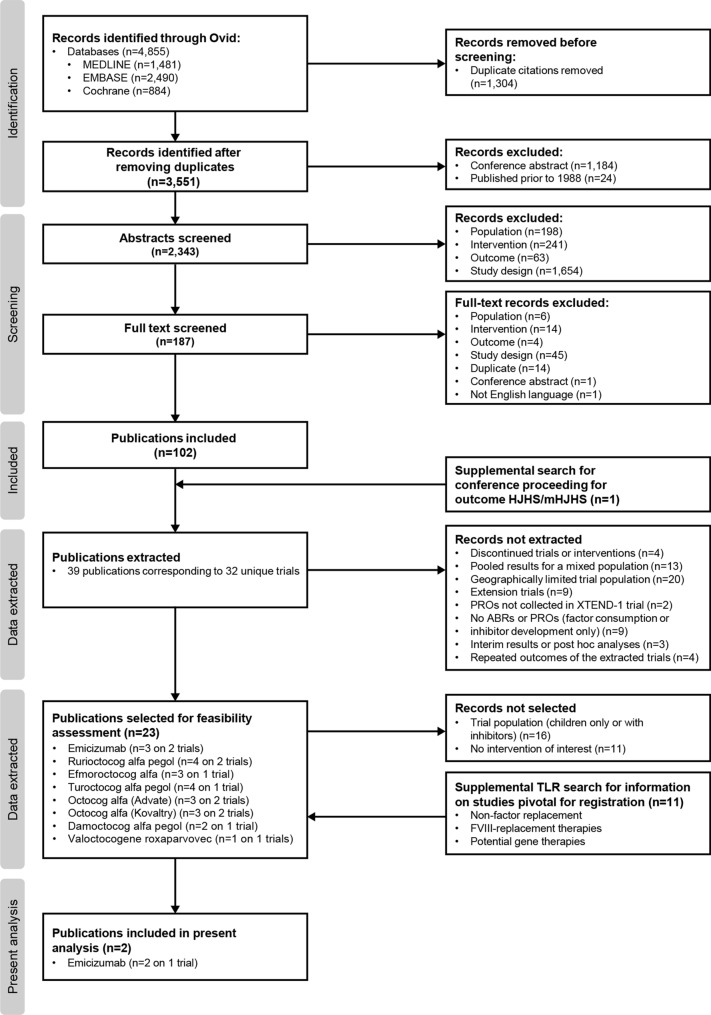
Methods: A systematic literature review was conducted to identify phase 3 trials of emicizumab. Matching-adjusted indirect comparisons were used to compare annualised bleeding rates (ABRs) for any, treated, joint, and spontaneous bleeds, and joint health (measured using Hemophilia Joint Health Score [HJHS]), between efanesoctocog alfa and emicizumab. Estimated effects for different emicizumab regimens were pooled using random-effect meta-analysis to evaluate the overall difference in bleed outcomes between efanesoctocog alfa and emicizumab.
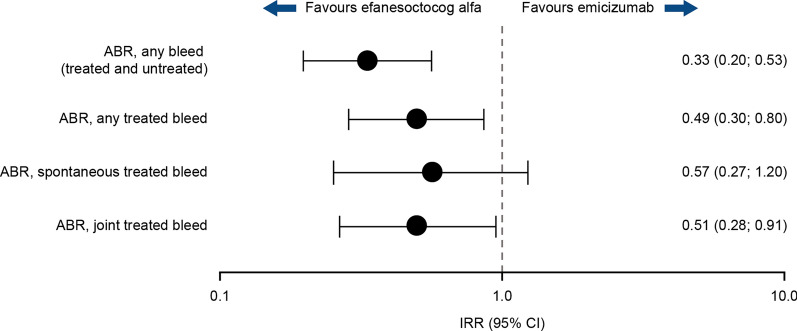
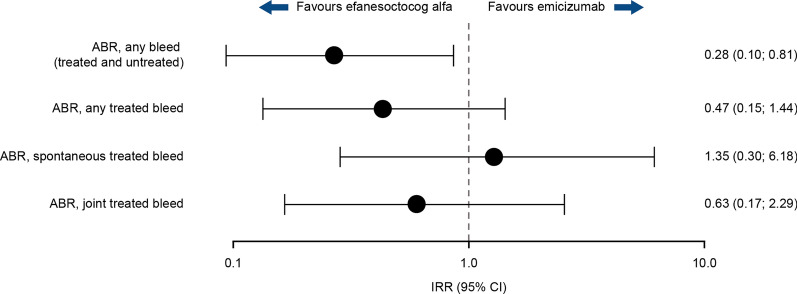
Results: One emicizumab trial was included (HAVEN 3), which investigated three dosing regimens. In meta-analyses, efanesoctocog alfa once-weekly (Q1W) was associated with significantly lower ABRs for any (incidence rate ratio [95% CI] 0.33 [0.20; 0.53]), any treated (0.49 [0.30; 0.80]) and treated joint (0.51 [0.28; 0.91]) bleeds compared with emicizumab Q1W in non-inhibitor patients with prior prophylaxis or on-demand treatment. Efanesoctocog alfa Q1W was also associated with a significantly better improvement from baseline in HJHS Joint Score (mean difference [95% CI] -2.06 [-3.97; -0.14]) and Total Score (-2.37 [-4.36; -0.39]) versus emicizumab Q1W or every 2 weeks.
Conclusion: Efanesoctocog alfa prophylaxis was associated with significantly lower rates of any, treated, and joint bleeds and improved joint health compared with emicizumab in patients with severe haemophilia A.
Keywords: Annualised bleeding rate; Efanesoctocog alfa; Emicizumab; Factor VIII; Haemophilia A; Indirect treatment comparison.
Plain language summary
It is recommended that people with haemophilia A are treated prophylactically (treatment given regularly to prevent bleeding) with factor VIII (FVIII) replacement therapies or a non-factor replacement therapy called emicizumab. People with haemophilia who receive emicizumab may still have bleeds that need to be treated with additional FVIII therapy. In the XTEND-1 clinical trial, patients given efanesoctocog alfa, a new FVIII replacement therapy, had fewer bleeds than they did on the preventive therapy received before the trial. However, efanesoctocog alfa has not been compared with emicizumab. Researchers searched medical journals to identify clinical trials of emicizumab. They compared the number of bleeds and health status of joints in patients treated with efanesoctocog alfa in the XTEND-1 trial with patients treated with emicizumab in HAVEN 3, the trial found in the literature search. The results were analysed to find the overall difference between efanesoctocog alfa and emicizumab. Compared with once-weekly emicizumab, once-weekly efanesoctocog alfa reduced the number of overall bleeds, treated bleeds (additional therapy given to stop the bleeding), and treated joint bleeds. Patients who received efanesoctocog alfa also showed more joint health improvement over the treatment course than those given emicizumab either once-weekly or every 2 weeks. Efanesoctocog alfa may work better at preventing bleeds and improving joint health than the non-factor replacement therapy emicizumab. However, there were some differences between the groups of patients studied in the two trials.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: Alix Arnaud, Amanda Wilson, and Patricia Guyot are Sanofi employees and may hold stock/stock options in Sanofi. Nana Kragh and Elena Santagostino are employees of Sobi and may hold stock/stock options in Sobi. Marlena Wdowiak and Wojciech Margas are employees of Putnam PHMR. Piotr Wojciechowski is a co-founder of Assignity and an external consultant at Putnam PHMR. María Teresa Álvarez Román has received reimbursement for attending symposia/congresses and/or honoraria for speaking and/or honoraria for consulting, and/or funds for research from Takeda, Bayer, CSL-Behring, Novo Nordisk, Sobi, Roche, Biomarin, Novartis, Amgen, and Pfizer. Piotr Wojciechowski’s and Wojciech Margas’ affiliation Assignity is now called Clever-Access. Ethical Approval: This is a post hoc analysis and modelling of data already collected and/or published data. Original studies were all approved by the relevant institutional review boards at each study site and were carried out in accordance with the International Conference on Harmonisation good clinical practice guidelines and the Declaration of Helsinki.
Figures


References
-
- Srivastava A, Santagostino E, Dougall A, et al. WFH guidelines for the management of haemophilia, 3rd edition. Haemophilia. 2020;26(Suppl 6):1–158. - PubMed
-
- United States Food & Drug Administration. HEMLIBRA Full Prescribing Information. 2017. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/761083s000lbl.pdf. Accessed July 2024.
-
- European Medicines Agency. HEMLIBRA Summary of Product Characteristics. 2018. https://www.ema.europa.eu/en/documents/product-information/hemlibra-epar.... Accessed July 2024.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
