

Functional anatomy of the subthalamic nucleus and the pathophysiology of cardinal features of Parkinson's disease unraveled by focused ultrasound ablation
- PMID: 39576853
- PMCID: PMC11584003
- DOI: 10.1126/sciadv.adr9891
Functional anatomy of the subthalamic nucleus and the pathophysiology of cardinal features of Parkinson's disease unraveled by focused ultrasound ablation
Abstract
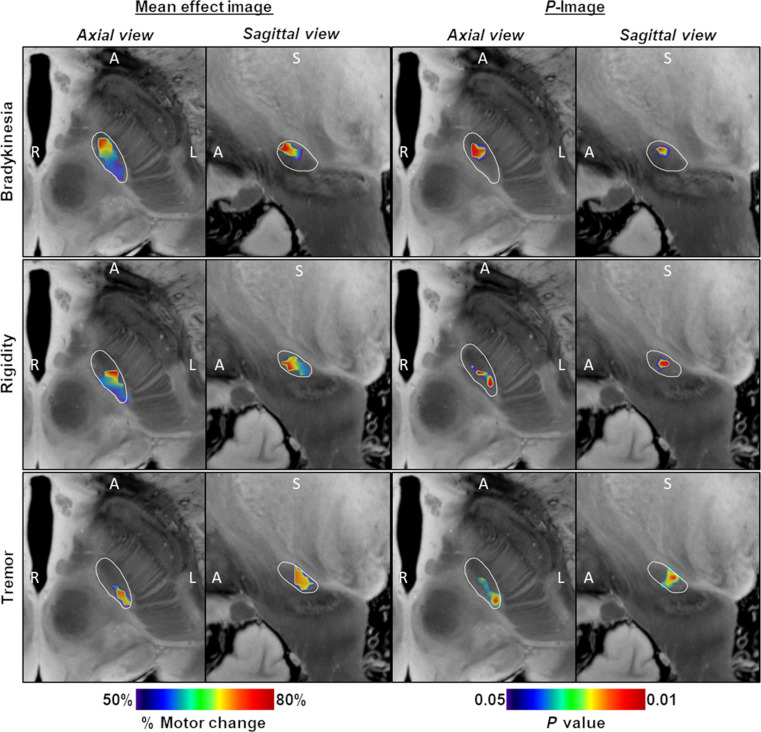
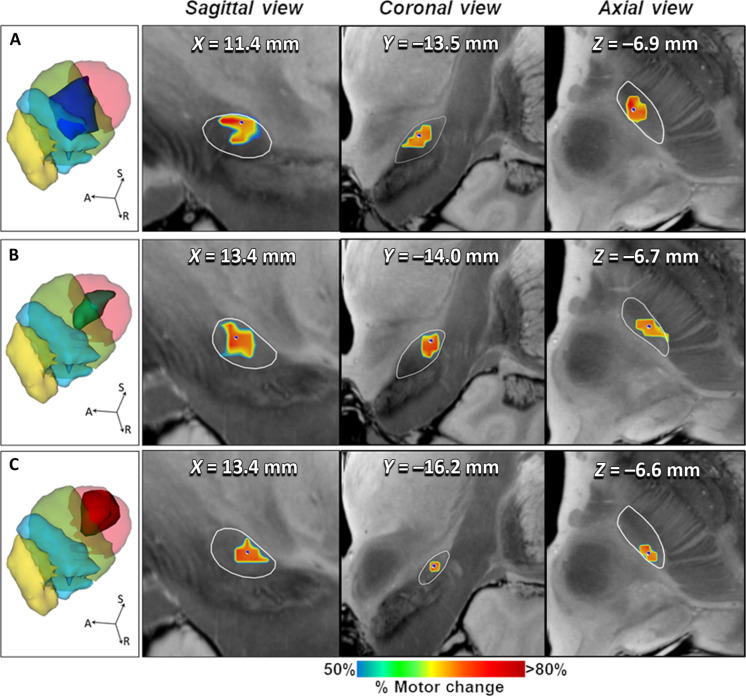
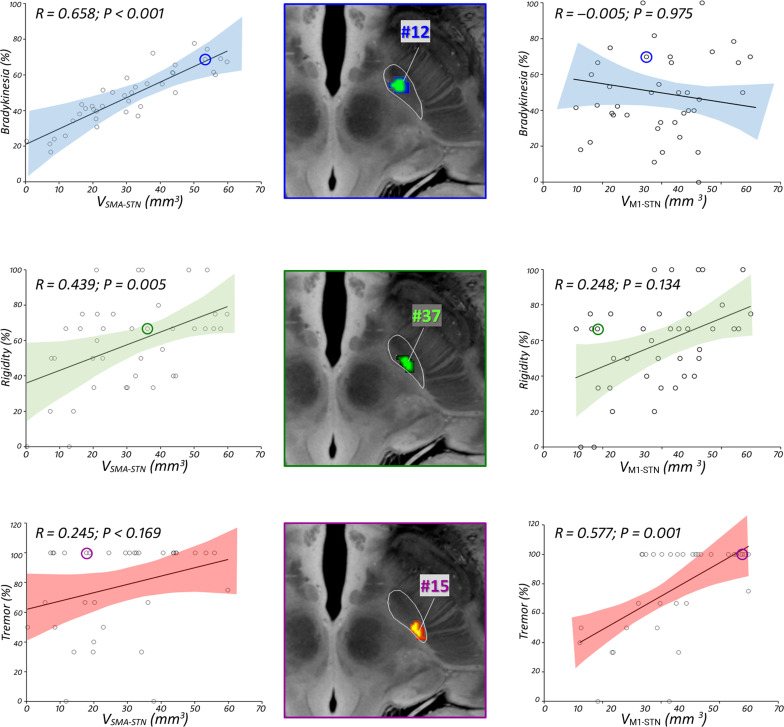
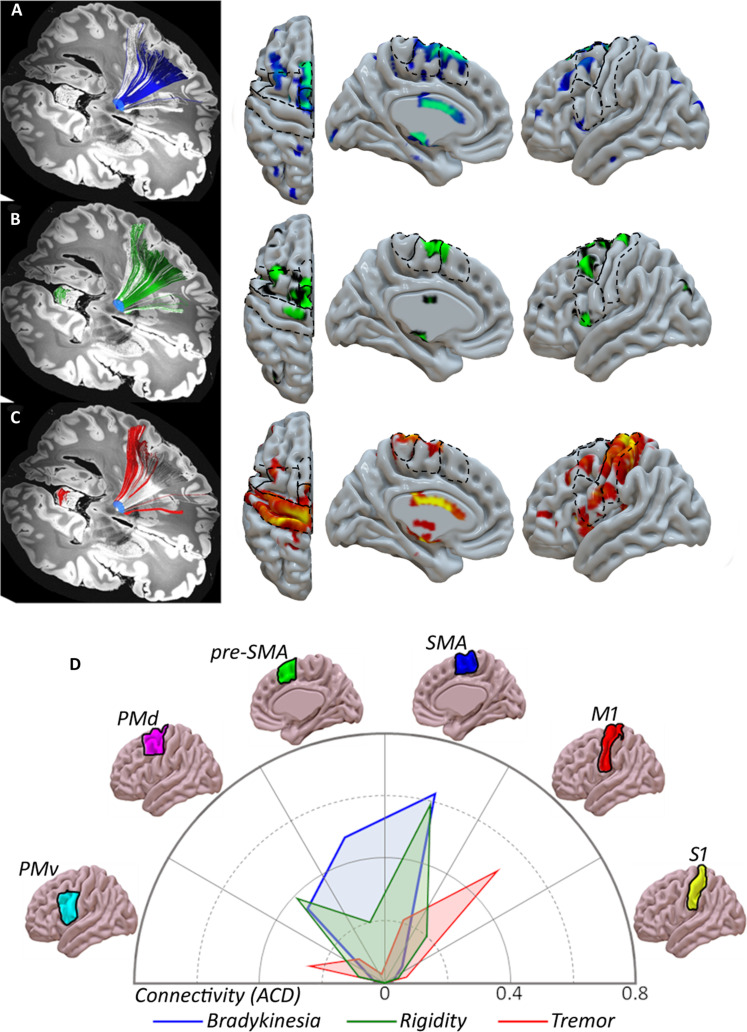
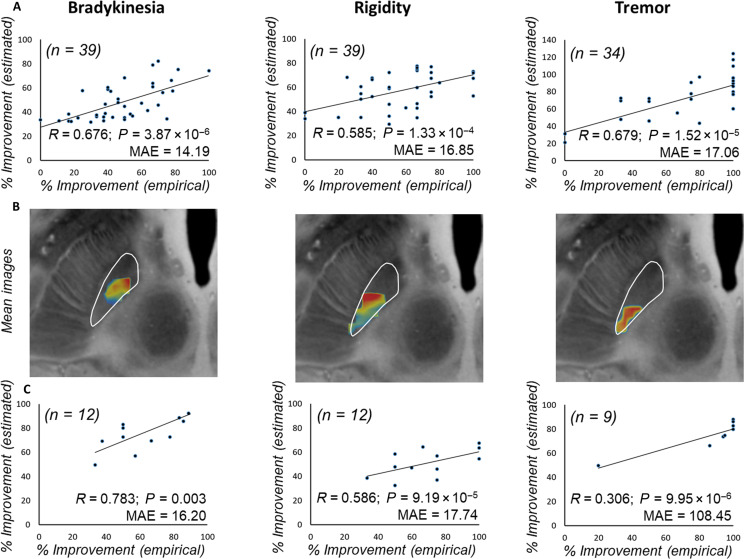
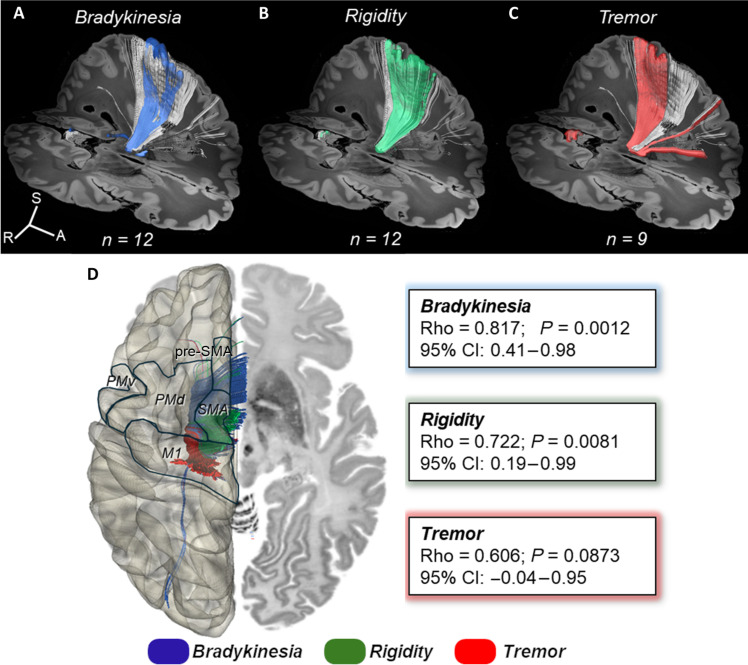
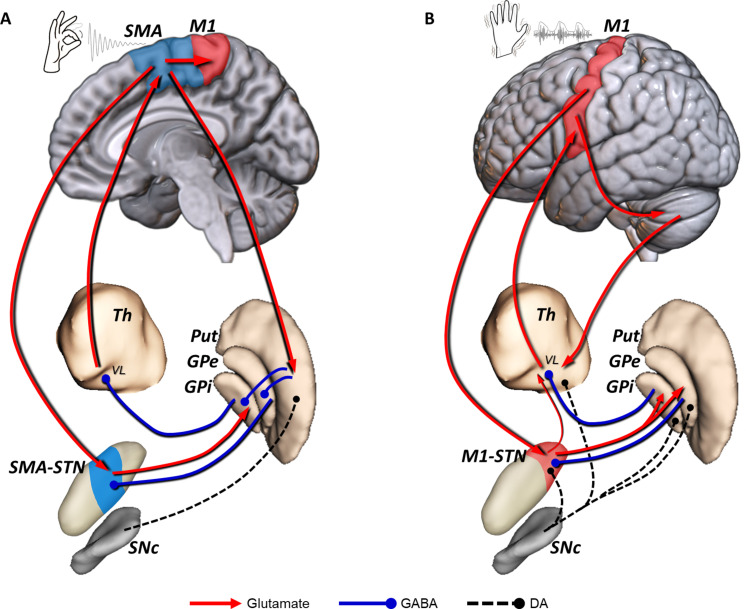
The subthalamic nucleus (STN) modulates basal ganglia output and plays a fundamental role in the pathophysiology of Parkinson's disease (PD). Blockade/ablation of the STN improves motor signs in PD. We assessed the topography of focused ultrasound subthalamotomy (n = 39) by voxel-based lesion-symptom mapping to identify statistically validated brain voxels with the optimal effect against each cardinal feature and their respective cortical connectivity patterns by diffusion-weighted tractography. Bradykinesia and rigidity amelioration were associated with ablation of the rostral motor STN subregion connected to the supplementary motor and premotor cortices, whereas antitremor effect was explained by lesioning the posterolateral STN projection to the primary motor cortex. These findings were corroborated prospectively in another PD cohort (n = 12). This work concurs with recent deep brain stimulation findings that suggest different corticosubthalamic circuits underlying each PD cardinal feature. Our results provide sound evidence in humans of segregated anatomy of subthalamic-cortical connections and their distinct role in PD pathophysiology and normal motor control.
Figures
References
-
- DeLong M. R., Wichmann T., Basal ganglia circuits as targets for neuromodulation in Parkinson disease. JAMA Neurol. 72, 1354–1360 (2015). - PubMed
-
- Krack P., Volkmann J., Tinkhauser G., Deuschl G., Deep brain stimulation in movement disorders: From experimental surgery to evidence-based therapy. Mov. Disord. 34, 1795–1810 (2019). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
