

Brain magnetic resonance imaging of patients with spinal muscular atrophy type 2 and 3
- PMID: 39577334
- PMCID: PMC11617753
- DOI: 10.1016/j.nicl.2024.103708
Brain magnetic resonance imaging of patients with spinal muscular atrophy type 2 and 3
Abstract
Background and objective: Proximal spinal muscular atrophy (SMA) is caused by deficiency of the ubiquitously expressed survival motor neuron protein. Although primarily a hereditary lower motor neuron disease, it is probably also characterized by abnormalities in other organs. Brain abnormalities and cognitive impairment have been reported in severe SMA. We aimed to systematically investigate brain structure in SMA using MRI.
Methods: We acquired high-resolution T1-weighted images of treatment-naive patients with SMA, age- and sex-matched healthy and disease controls with other neuromuscular diseases, on a 3 T MRI scanner. We performed vertex-wise whole brain analysis and region of interest analysis of cortical thickness (CT), and volumetric analysis of the thalamus and compared findings in patients and controls using multiple linear regression models and Wald test. We correlated structural abnormalities with motor function as assessed by the Hammersmith Functional Motor Scale Expanded (HFMSE) and SMA Functional Rating Scale (SMA-FRS).
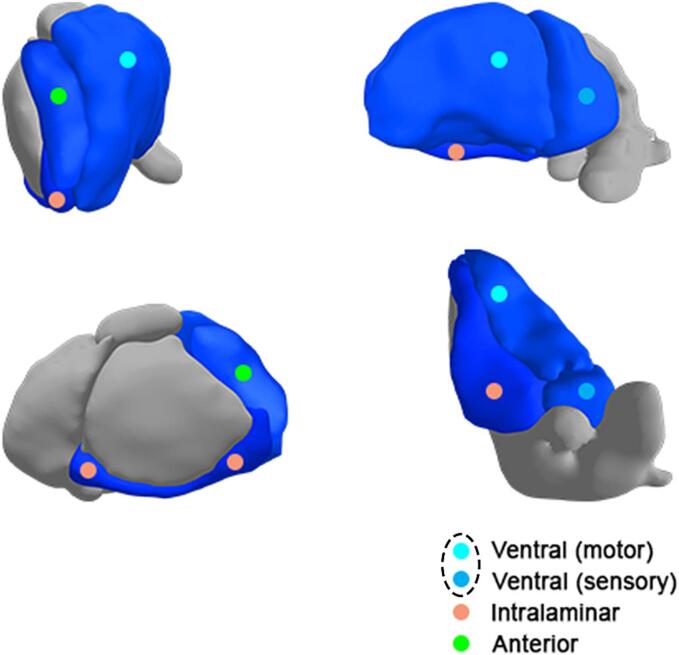
Results: We included 30 patients, 12-70 years old, with SMA type 2 and 3, 30 age- and sex-matched healthy controls and 17 disease controls (with distal SMA, hereditary motor and sensory neuropathy, multifocal motor neuropathy, progressive muscular atrophy and segmental SMA). We found a reduced CT in patients with SMA compared to healthy controls at the precentral, postcentral and medial orbitofrontal gyri and at the temporal pole (mean differences -0.059(p = 0.04); -0.055(p = 0.04), -0.06(p = 0.04); -0.17 mm(p = 0.001)). Differences at the precentral gyrus and temporal pole were most pronounced in SMA type 2 (mean differences -0.07(p = 0.045); -0.26 mm(p < 0.001)) and were also present compared to disease controls (mean differences -0.08(p = 0.048); -0.19 mm(p = 0.003)). There was a positive correlation between CT at the temporal pole with motor function. Compared to healthy controls, we found a reduced volume of the whole thalamus (mean difference -325 mm3(p = 0.03)) and of the anterior, ventral and intralaminar thalamic nuclei (mean differences -9.9(p = 0.02); -157(p = 0.01); -24.2 mm3(p = 0.02) in patients with SMA and a positive correlation between these volumes and motor function.
Conclusion: MRI shows structural changes in motor and non-motor regions of the cortex and the thalamus of patients with SMA type 2 and 3, indicating that SMA pathology is not confined to motor neurons.
Keywords: Brain; Cortical thickness; MRI; SMA; Spinal muscular atrophy; Thalamus.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: [Martijn P. van den Heuvel works as a consultant for ROCHE and is part of the editorial board of Human Brain Mapping. Leonard H. van den Berg serves on scientific advisory boards for the Prinses Beatrix Spierfonds and receives research support from the Prinses Beatrix Fonds. W. Ludo van der Pol served as an ad hoc member of scientific advisory boards (fee for service to employer) for Biogen, Biohaven, NMD Pharma, Scholar Rock, Roche and Novartis Genetherapies and receives research support from the Prinses Beatrix Spierfonds, EU Horizon 2020, Vriendenloterij and Stichting Spieren voor Spieren. Marloes Stam, Harold H. G. Tan, Ruben Schmidt and Renske I. Wadman report no competing interests].
Figures






References
-
- The ALS CNTF treatment study (ACTS) phase I-II Study Group. The Amyotrophic Lateral Sclerosis Functional Rating Scale. Assessment of activities of daily living in patients with amyotrophic lateral sclerosis. Arch Neurol. 1996; 53:141–147. - PubMed
-
- Araki S., Hayashi M., Tamagawa K., et al. Neuropathological analysis in spinal muscular atrophy type II. Acta Neuropathol. 2003;106:441–448. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
