

Sensitivity and specificity of a seed amplification assay for diagnosis of multiple system atrophy: a multicentre cohort study
- PMID: 39577923
- PMCID: PMC12288831
- DOI: 10.1016/S1474-4422(24)00395-8
Sensitivity and specificity of a seed amplification assay for diagnosis of multiple system atrophy: a multicentre cohort study
Abstract
Background: The pathological hallmarks of multiple system atrophy and Parkinson's disease are, respectively, misfolded-α-synuclein-laden glial cytoplasmic inclusions and Lewy bodies. CSF-soluble misfolded α-synuclein aggregates (seeds) are readily detected in people with Parkinson's disease by α-synuclein seed amplification assay (synSAA), but identification of seeds associated with multiple system atrophy for diagnostic purposes has proven elusive. We aimed to assess whether a novel synSAA could reliably distinguish seeds from Lewy bodies and glial cytoplasmic inclusions.
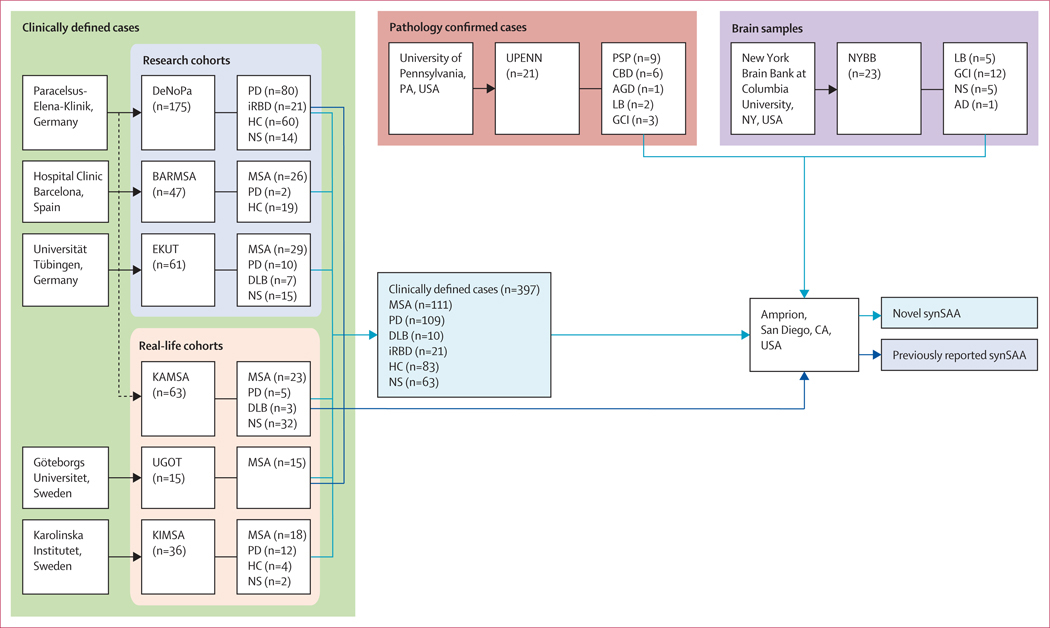
Methods: In this multicentre cohort study, a novel synSAA that multiplies and detects seeds by fluorescence was used to analyse masked CSF and brain samples from participants with either clinically diagnosed or pathology-confirmed multiple system atrophy, Parkinson's disease, dementia with Lewy bodies, isolated rapid eye movement sleep behaviour disorder (IRBD), disorders that were not synucleinopathies, or healthy controls. Participants were from eight available cohorts from seven medical centres in four countries: New York Brain Bank, New York, USA (NYBB); University of Pennsylvania, Philadelphia, PA, USA (UPENN); Paracelsus-Elena-Klinik, Kassel, Germany (DeNoPa and KAMSA); Hospital Clinic Barcelona, Spain (BARMSA); Universität Tübingen, Tübingen, Germany (EKUT); Göteborgs Universitet, Göteborgs, Sweden (UGOT); and Karolinska Institutet, Stockholm, Sweden (KIMSA). Clinical cohorts were classified for expected diagnostic accuracy as either research (longitudinal follow-up visits) or real-life (single visit). Sensitivity and specificity were estimated according to pathological (gold standard) and clinical (reference standard) diagnoses.
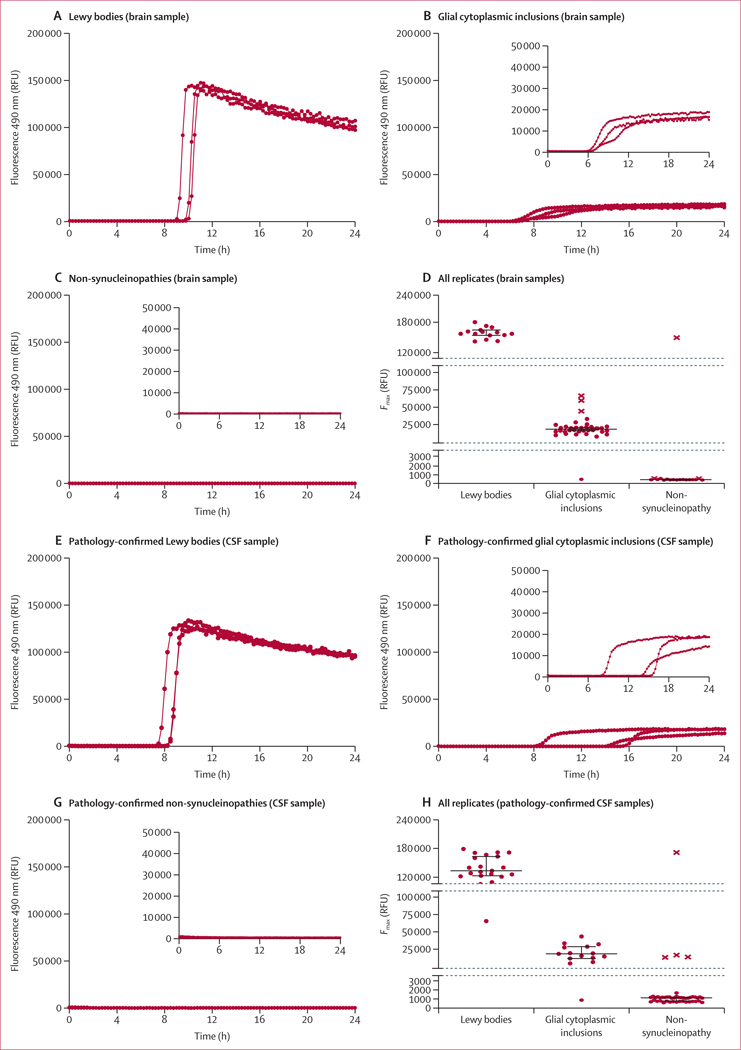
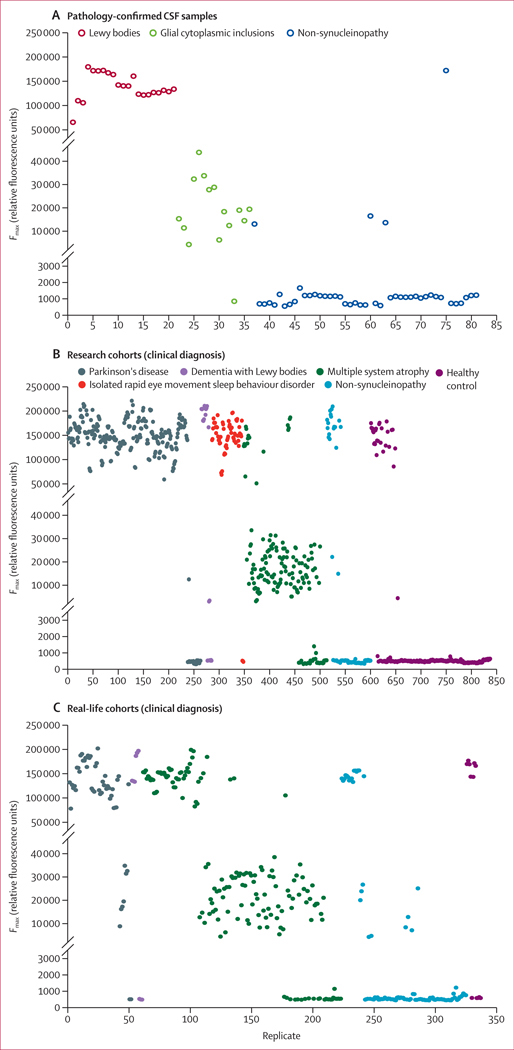
Findings: In 23 brain samples (from the NYBB cohort), those containing Lewy bodies were synSAA-positive and produced high fluorescence amplification patterns (defined as type 1); those containing glial cytoplasmic inclusions were synSAA-positive and produced intermediate fluorescence (defined as type 2); and those without α-synuclein pathology produced below-threshold fluorescence and were synSAA-negative. In 21 pathology-confirmed CSF samples (from the UPENN cohort), those with Lewy bodies were synSAA-positive type 1; those with glial cytoplasmic inclusions were synSAA-positive type 2; and those with four-repeat tauopathy were synSAA-negative. In the DeNoPa research cohort (which had no samples from people with multiple system atrophy), the novel synSAA had sensitivities of 95% (95% CI 88-99) for 80 participants with Parkinson's disease and 95% (76-100) for 21 participants with IRBD, and a specificity of 95% (86-99) for 60 healthy controls. Overall (combining BARMSA, EKUT, KAMSA, UGOT, and KIMSA cohorts that were enriched for cases of multiple system atrophy), the novel synSAA had 87% sensitivity for multiple system atrophy (95% CI 80-93) and specificity for type 2 seeds was 77% (67-85). For participants with multiple system atrophy just in research cohorts (BARMSA and EKUT), the novel synSAA had a sensitivity of 84% (95% CI 71-92) and a specificity for type 2 seeds of 87% (74-95), whereas cases from real-life cohorts (KAMSA, KIMSA, and UGOT) had a sensitivity of 91% (95% CI 80-97) but a decreased specificity for type 2 seeds of 68% (53-81).
Interpretation: The novel synSAA produced amplification patterns that enabled the identification of underlying α-synuclein pathology, showing two levels of fluorescence that corresponded with different pathological hallmarks of synucleinopathy. The synSAA might be useful for early diagnosis of synucleinopathies in clinical trials, and potentially for clinical use, but additional formal validation work is needed.
Funding: Michael J Fox Foundation for Parkinson's Research, Amprion.
Copyright © 2024 Elsevier Ltd. All rights reserved, including those for text and data mining, AI training, and similar technologies.
Conflict of interest statement
Declaration of interests YM, CMF, HN, and LC-M are Amprion employees and declare employee stock option ownership and invention of patents related to SAA assigned to Amprion. YM declares patent or patent application numbers US11970520B2, US20230084155A1. CMF declares patent or patent application numbers US11970520B2, US11959927B2, and US20230084155A1. HN declares patent or patent application numbers US20230084155A1. LC-M declares patent or patent application numbers US11970520B2, US11959927B2, US20190353669A1, US20230084155A1, and US20210223268A1. UJK is on the scientific advisory board of Amprion, on the data monitoring committee for UCB, and a consultant for NurrOn. MSy has received consultancy honoraria from Ionis, UCB, Prevail, Orphazyme, Servier, Reata, GenOrph, AviadoBio, Biohaven, Zevra, Solaxa, and Lilly, all unrelated to the present manuscript. HZ has served at scientific advisory boards or as a consultant, or both, for Abbvie, Acumen, Alector, Alzinova, ALZPath, Amylyx, Annexon, Apellis, Artery Therapeutics, AZTherapies, Cognito Therapeutics, CogRx, Denali, Eisai, Merry Life, Nervgen, Novo Nordisk, Optoceutics, Passage Bio, Pinteon Therapeutics, Prothena, Red Abbey Labs, reMYND, Roche, Samumed, Siemens Healthineers, Triplet Therapeutics, and Wave; has given lectures in symposia sponsored by Alzecure, Biogen, Cellectricon, Fujirebio, Lilly, Novo Nordisk, and Roche; is chair of the Alzheimer's Association Global Biomarker Standardization Consortium; and is a co-founder of Brain Biomarker Solutions in Gothenburg, which is a part of the GU Ventures Incubator Program. RNA received consultation fees from Biogen, Biohaven, Capsida, Gain Therapeutics, Genzyme/Sanofi, Servier, Takeda, and Vanqua Bio. TFT serves as a clinical trial advisory board member for Bial. KBr is on the advisory boards of F Hoffman La Roche, VanquaBio, and the Michael J Fox Foundation. PS is a DSMB member in Amulet study in MSA for Lundbeck. BM has received honoraria for consultancy or educational presentations, or both, from GE, Bial, Roche, Biogen, and AbbVie, and is member of the executive steering committee of the Parkinson Progression Marker Initiative of the Michael J Fox Foundation for Parkinson's Research and has received research funding from Aligning Science Across Parkinson's disease Collaborative Research Network. CP has received honoraria financed by Bial. AS declares consultancy for Acadia, Boehringer-Ingelheim, Mitzubishi, GE Healthcare, and Capsida. AS declares participation on a data safety monitoring board or advisory board for Wave Life Sciences, Inhibikase, Prevail, Alterity, Healy ALS Consortium (Massachusetts General Hospital), and Huntington Study Group. KBl has served as a consultant or on an advisory board for Abbvie, AriBio, ALZpath, BioArctic, AC Immune, Biogen, Eisai, Lilly, Ono Pharma, Prothena, Roche Diagnostics, and Siemens Healthineers, and produced or participated in educational programmes for Biogen, Eisai, and Roche Diagnostics.
Figures
References
-
- Tu PH, Galvin JE, Baba M, et al. Glial cytoplasmic inclusions in white matter oligodendrocytes of multiple system atrophy brains contain insoluble alpha-synuclein. Ann Neurol 1998; 44: 415–22. - PubMed
-
- Osaki Y, Ben-Shlomo Y, Lees AJ, Wenning GK, Quinn NP. A validation exercise on the new consensus criteria for multiple system atrophy. Mov Disord 2009; 24: 2272–76. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
