

Postpartum maternal and infant haematological effects of second-trimester ferric carboxymaltose versus standard-of-care oral iron in Malawi: longitudinal follow-up of a randomised controlled trial
- PMID: 39577976
- PMCID: PMC11584314
- DOI: 10.1016/S2214-109X(24)00380-2
Postpartum maternal and infant haematological effects of second-trimester ferric carboxymaltose versus standard-of-care oral iron in Malawi: longitudinal follow-up of a randomised controlled trial
Abstract
Background: Anaemia is common in mothers and infants in the first year postpartum, especially in sub-Saharan Africa. We evaluated whether treating anaemia in the second trimester of pregnancy with a single dose of intravenous iron, ferric carboxymaltose, compared with standard-of-care oral iron could alleviate anaemia in postpartum women and their infants.
Methods: REVAMP (ACTRN12618001268235), an open-label, individually randomised, controlled trial done across nine urban and five rural health centres in Malawi, recruited women if they were in the second trimester of singleton pregnancy, had a capillary haemoglobin concentration of less than 10·0 g/dL, and had a negative malaria rapid diagnostic test. Once enrolled, women were randomly assigned (1:1) to receive intravenous ferric carboxymaltose (20 mg/kg up to 1000 mg) or standard of care (60 mg oral elemental iron twice daily for 90 days); all women received preventive malaria treatment. The primary endpoint of REVAMP was anaemia prevalence at 36 weeks of gestation, with follow-up of mothers and infants until 1 month postpartum. In REVAMP-EXTENDED, women from REVAMP who gave consent, and their infants, were followed up at 3, 6, 9, and 12 months postpartum, and venous blood was collected for haemoglobin, ferritin, and C-reactive protein measurement. Maternal postpartum outcomes comprised prevalence of anaemia (venous haemoglobin concentration <11 g/dL up to and including delivery and <12·0 g/dL postpartum) and haemoglobin concentration, as well as iron status (iron deficiency, defined as serum ferritin <15 μg/L, or <30 μg/L if C-reactive protein >5 mg/L, and iron deficiency anaemia [both iron deficiency and anaemia]). Infant outcomes comprised cord ferritin concentration, and haemoglobin and ferritin concentrations at 1, 3, 6, 9, and 12 months of age.
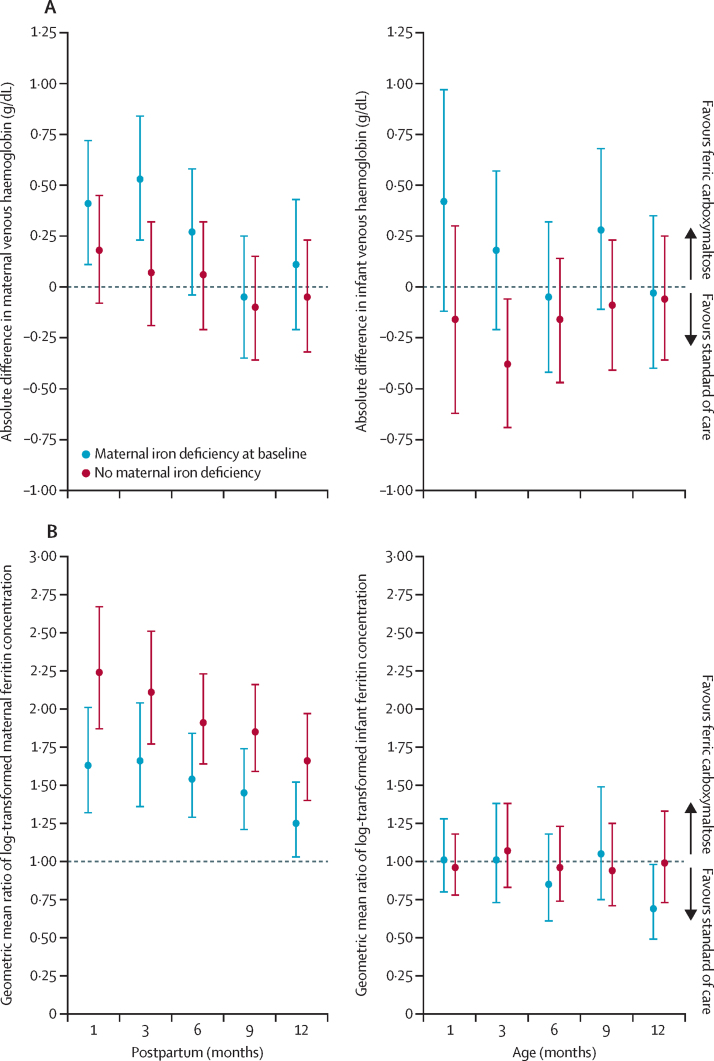
Findings: Between Nov 12, 2018, and March 2, 2021, 862 women were randomly assigned in REVAMP, of whom 793 (393 in the ferric carboxymaltose group [376 liveborn infants] and 400 [379 liveborn infants] in the standard-of-care group) provided consent for REVAMP-EXTENDED. At 12 months postpartum, ferritin concentrations were higher (geometric mean ratio 1·47 [95% CI 1·29-1·66], p<0·0001), and prevalence of iron deficiency was lower (prevalence ratio 0·65 [0·48-0·88], p=0·0050), in mothers receiving ferric carboxymaltose than in those receiving standard of care. Anaemia was less common in women who received ferric carboxymaltose than in those who received standard of care at 1 month (prevalence ratio 0·84 [95% CI 0·71-0·98], p=0·027), 3 months (0·75 [0·62-0·91], p=0·0029), and 6 months (0·78 [0·63-0·96], p=0·018) postpartum but not thereafter. There was no evidence of a difference between groups regarding cord ferritin, infant ferritin, or infant haemoglobin concentrations at any timepoint. Benefits on postpartum anaemia were restricted to mothers with baseline iron deficiency.
Interpretation: Ferric carboxymaltose treatment in the second trimester protected women from postpartum anaemia and iron deficiency but did not affect infant haematological or iron status.
Funding: Bill & Melinda Gates Foundation.
Translation: For the Chichewa translation of the abstract see Supplementary Materials section.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests S-RP reports grants to his institution from the Australian National Health and Medical Research Council and the Bill & Melinda Gates Foundation, providing salary and research support; paid advisory board roles for CSL-Vifor for iron and immunity and for vamifeport in sickle cell disease; consultancy for ITL Biomedical on point-of-care devices in iron; research support from WHO; and unpaid roles as Director (WHO Collaborating Centre for Anaemia Detection and Control) and as co-Chair (Guideline Development Group Meetings). RA owns stock in CSL-Vifor (manufacturer of ferric carboxymaltose). All other authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
