

High flow nasal cannula and low level continuous positive airway pressure have different physiological effects during de novo acute hypoxemic respiratory failure
- PMID: 39578265
- PMCID: PMC11584821
- DOI: 10.1186/s13613-024-01408-w
High flow nasal cannula and low level continuous positive airway pressure have different physiological effects during de novo acute hypoxemic respiratory failure
Abstract
Background: Large tidal volumes during de novo acute hypoxemic respiratory failure (AHRF) may promote patient self-inflicted lung injury. Tidal volume assessment under high flow nasal cannula (HFNC) is not routinely feasible at the bedside. Our objective was to determine whether tidal volume during low-level continuous positive airway pressure (CPAP) could predict tidal volume during HFNC and to compare the physiological effects of HFNC and low-level CPAP.
Methods: Prospective, single-center study including 29 de novo AHRF patients treated with HFNC (50 to 60 L.min- 1). Patients were monitored using electrical impedance tomography during HFNC then CPAP at 4 cmH2O. Tidal volume during HFNC was calculated based on tidal impedance variation. The ability of tidal volume under low-level CPAP to predict tidal volume under HFNC was explored using Bland-Altman analysis. CPAP and HFNC were compared in terms of tidal volume, minute ventilation, respiratory comfort, dyspnea, oxygenation, ventilation distribution, end-expiratory lung volume, thoraco-abdominal asynchrony and recruitment.
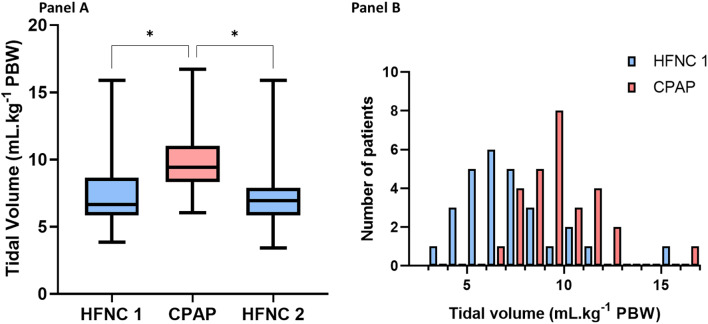
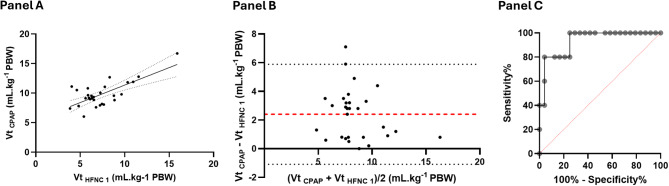
Results: Under HFNC, patients had a tidal volume of 6.6 (5.9-8.7) mL.kg- 1 PBW. 20 (69%) patients exhibited a tidal volume between 4 and 8 mL.kg- 1 PBW, while in 5 (17%) patients it exceeded 9 mL.kg- 1 PBW. Tidal volume under CPAP was higher (9.4 (8.3-11) mL.kg- 1 PBW, p < 0.001). Tidal volumes under CPAP and under HFNC were modestly correlated (Spearman r = 0.50, p = 0.005). Bland-Altman analysis showed a bias of 2.4 mL.kg- 1, with limits of agreement ranging from - 1.1 mL.kg- 1to 5.9 mL.kg- 1. Nevertheless, a larger (> 11.5 mL.kg- 1 PBW ) tidal volume under low-level CPAP predicted a larger (> 9 mL.kg- 1 PBW ) tidal volume under HFNC with 80% sensitivity and 96% specificity. Low-level CPAP was associated with increased minute ventilation, end-expiratory lung volume, and oxygenation as compared to HFNC. It decreased signs of respiratory distress in the most severe patients but was associated with lower comfort compared to HFNC.
Conclusion: Among ICU patients with de novo AHRF, tidal volume under HFNC was mostly protective. Tidal volume during CPAP at 4 cmH2O did not predict tidal volume during HFNC. Such low-level CPAP was associated with increased tidal volume, minute ventilation, end-expiratory volume, and oxygenation.
Trial registration: ClinicalTrials.gov ID NCT03919331. Registration date: 2019-03-26.
Keywords: Acute hypoxemic respiratory failure; Continuous positive airway pressure; High flow nasal cannula; Noninvasive ventilation; Respiratory support.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by an ethic committee “Comité de Protection des Personnes Ile de France 4” (2018-A02972-53). All participants received oral and written information and signed a consent form. Consent for publication: NA. Competing interests: AF. Haudebourg reports personal fees from Air Liquide Medical System, Drager, Medtronic and Fisher & Paykel, outside the submitted work. A. Mekontso Dessap reports grants from Fisher and Paykel and fees fom Air Liquide Medical System and Fisher and Paykel, outside the submitted work. G. Carteaux reports grant from Hamilton, personal fees from Air Liquide Medical System, GE Healthcare, Dräger, Fisher and Paykel, Medtronic and Löwenstein, outside the submitted work. Samuel Tuffet, Mohamed Ahmed Boujelben, Tommaso Maraffi, François Perier, Pascale Labedade, Elsa Moncomble, Ségolène Gendreau, Matthieu Lacheny and Emmanuel Vivier report no competing interest.
Figures
References
-
- Carteaux G, Millán-Guilarte T, De Prost N, Razazi K, Abid S, Thille AW, et al. Failure of noninvasive ventilation for De Novo Acute Hypoxemic Respiratory failure: role of tidal Volume*. Crit Care Med. 2016;44(2):282–90. - PubMed
-
- Frat JP, Ragot S, Coudroy R, Constantin JM, Girault C, Prat G, et al. Predictors of intubation in patients with Acute Hypoxemic respiratory failure treated with a Noninvasive Oxygenation Strategy*. Crit Care Med. 2018;46(2):208–15. - PubMed
-
- Brochard L, Slutsky A, Pesenti A. Mechanical ventilation to minimize progression of Lung Injury in Acute Respiratory failure. Am J Respir Crit Care Med. 2017;195(4):438–42. - PubMed
-
- Carteaux G, Perier F, Maraffi T, Razazi K, De Prost N, Mekontso Dessap A. Patient self-inflicted lung injury: Ce que le réanimateur doit connaître. Méd Intensive Réa. 2019;28(1):11–20.
-
- Frat JP, Thille AW, Mercat A, Girault C, Ragot S, Perbet S, et al. High-Flow Oxygen through Nasal Cannula in Acute Hypoxemic Respiratory failure. N Engl J Med. 2015;372(23):2185–96. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
