

Real-world rates and risk factors for subsequent treatment with vertebroplasty or balloon kyphoplasty after initial vertebral augmentation: a retrospective cohort study
- PMID: 39578267
- PMCID: PMC11706842
- DOI: 10.1007/s00198-024-07294-z
Real-world rates and risk factors for subsequent treatment with vertebroplasty or balloon kyphoplasty after initial vertebral augmentation: a retrospective cohort study
Abstract
The purpose of this study was to determine the real-world incidence and predictors of additional vertebroplasty or balloon kyphoplasty after initial vertebral augmentation, as a proxy for subsequent symptomatic vertebral fracture. Of patients, 15.5% underwent subsequent vertebral augmentation. The patient's comorbidities are strongly associated with risk of subsequent treatment.
Purpose: To determine the real-world incidence and predictors of additional vertebroplasty or balloon kyphoplasty after initial vertebral augmentation, as a proxy for subsequent symptomatic and disabling vertebral fracture.
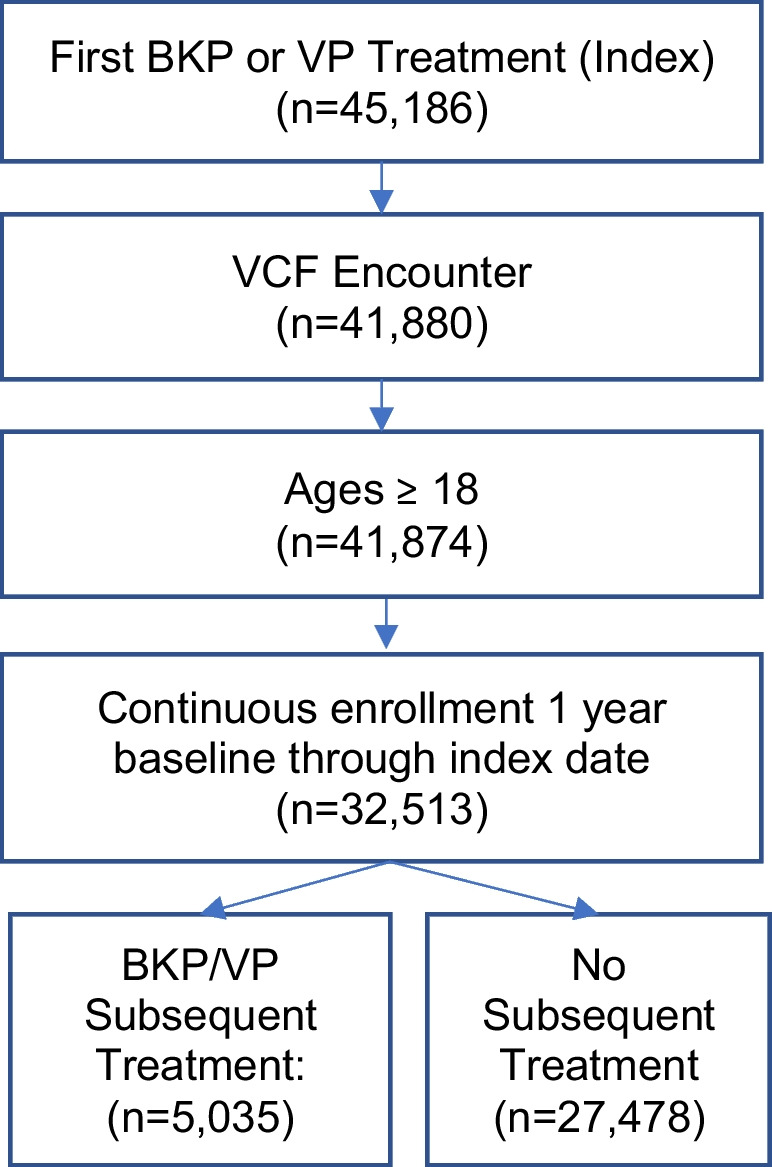
Methods: We conducted a retrospective cohort study using commercial insurance claims data (Optum's de-identified Clinformatics® Data Mart Database). Adult patients who underwent subsequent treatment for vertebral fracture within 24 months of initial balloon kyphoplasty (BKP) or vertebroplasty (VP) were classified into "subsequent treatment" or "no subsequent treatment" cohorts. Survival analysis was applied to investigate the effect of risk factors on subsequent treatment.
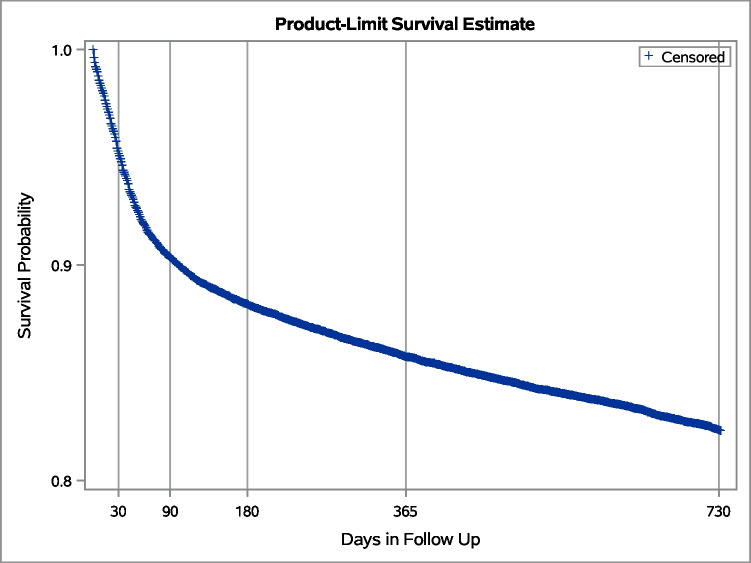
Results: Between 1 January 2008 and 30 June 2020, a total of 32,513 adult patients underwent a BKP/VP procedure following a diagnosis of vertebral compression fracture in the preceding 12 months. Five thousand thirty-five patients (15.5%) underwent a subsequent BKP/VP treatment within 2 years; 90% had a single fracture level treated. An increased hazard of subsequent treatment was associated with a number of fractures treated at initial BKP/VP (≥ 4 levels, adjusted hazard ratio (AHR) 1.68 (95% CI 1.24-2.26); steroid use, AHR 1.9 (95% CI 1.31-1.48); Elixhauser Comorbidity Index ≥ 4, AHR 1.44 (95% CI 1.17-1.77); and multiple myeloma, AHR 1.31 (95% CI 1.13-1.53)). Age < 70 years was associated with reduced hazard of subsequent treatment (AHR 0.81, 95% CI 0.74-0.89).
Conclusions: One in seven patients underwent subsequent treatment for vertebral fracture after initial vertebral augmentation. Baseline patient characteristics were associated with increased risk of subsequent fracture within 2 years, suggesting that a patient's natural history is strongly associated with risk of subsequent treatment rather than the initial surgical procedure itself.
Keywords: Balloon kyphoplasty; Osteoporosis; Subsequent fracture; Vertebral augmentation; Vertebral compression fracture; Vertebroplasty.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This was an observational study of de-identified data. Sterling IRB (Atlanta, GA, USA) has determined that the study is exempt from full IRB review. Formal consent for this retrospective study was not required. Sterling IRB (Atlanta, GA, USA) has determined that no patient consent to participate was required. Conflicts of interest: NCG, CNR and CW are current employees of Medtronic. JAH was a consultant for Medtronic, Relievant, and Cerenovus in the last 12 months, and provided DMC and DSMB chair work for Rapid Medical, Balt, and Arsenal in the last 12 months. JAH’s effort is supported in part by a grant from the Harvey L. Neiman Health Policy Institute. CG consulted for Mainstay, Persica, Saluda, Iliad Lifesciences, Biotronik, and Presidio; has stock options with Mainstay; is on the board of directors of the International Neuromodulation Society; and is Editor-in-Chief of Pain Practice. AB was an advisor for Medtronic, NEVRO, and Boston Scientific. RVC declares no competing interests.
Figures

References
-
- Cosman F, Krege JH, Looker AC et al (2017) Spine fracture prevalence in a nationally representative sample of US women and men aged ≥40 years: results from the National Health and Nutrition Examination Survey (NHANES) 2013–2014. Osteoporos Int 28:1857–1866. 10.1007/s00198-017-3948-9 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
