

Population Pharmacokinetics of Intravenous Paracetamol and Its Metabolites in Extreme Preterm Neonates in the Context of Patent Ductus Arteriosus Treatment
- PMID: 39578300
- PMCID: PMC11649743
- DOI: 10.1007/s40262-024-01439-3
Population Pharmacokinetics of Intravenous Paracetamol and Its Metabolites in Extreme Preterm Neonates in the Context of Patent Ductus Arteriosus Treatment
Abstract
Aims: Our aim was to describe the pharmacokinetics of paracetamol and its metabolites in extreme preterm neonates in the context of patent ductus arteriosus treatment. Factors associated with inter-individual variability and metabolic pathways were studied. The association between drug exposure and clinical outcomes were investigated.
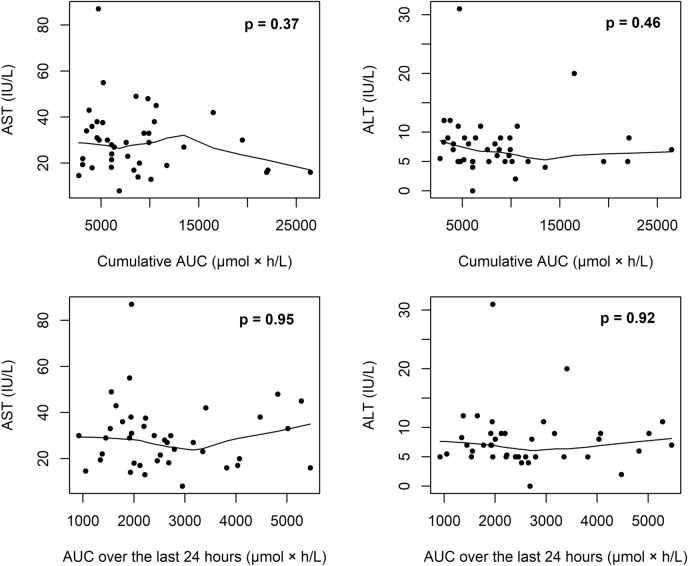
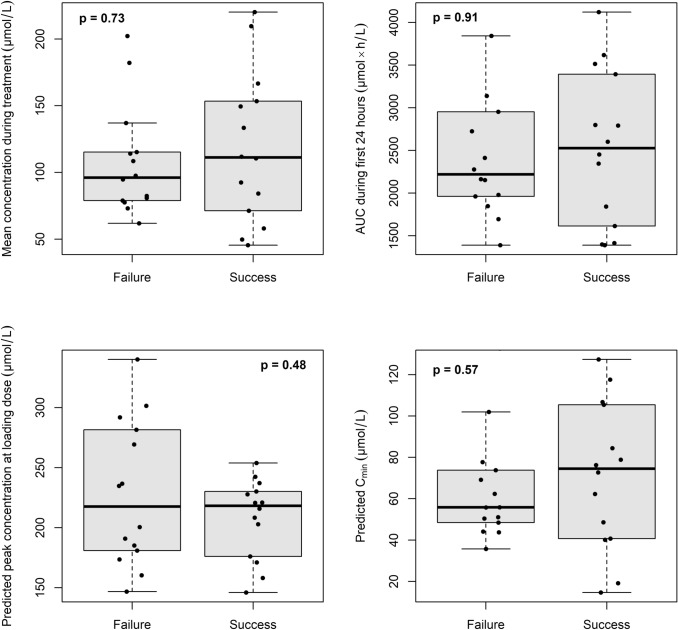
Methods: Preterm neonates of 23-26 weeks' gestational age received paracetamol within 12 h after birth. Plasma concentrations of paracetamol and its metabolites were measured throughout 5 days of treatment. Clinical success was defined as ductus closure on two consecutive days or at day 7. Aspartate aminotransferase and alanine aminotransferase levels were used as surrogates for liver damage.
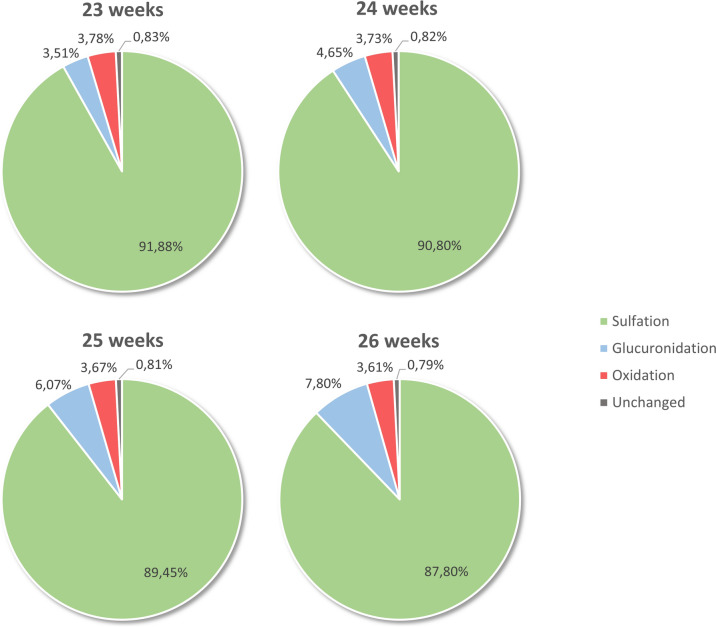
Results: Data from 30 preterm neonates were available for pharmacokinetic analysis. Paracetamol pharmacokinetics were described using a two-compartment model with significant positive effects of weight on clearance and of birth length on peripheral compartment volume. Paracetamol was mainly metabolised into sulphate (89%) then glucuronide (6%), and the oxidative metabolic pathway was reduced (4%). The glucuronidation pathway increased with gestational age, whereas the sulfation pathway decreased. No difference was observed in drug exposure between successful and unsuccessful patients. No increase in aspartate aminotransferase and alanine aminotransferase levels were observed during treatment, and no association was found with either paracetamol or oxidative metabolite exposures.
Conclusion: The relative proportions of the metabolic pathways were characterised with gestational age. In the range of observed drug exposures, no association was found with clinical response or liver biomarkers. These findings may suggest that paracetamol concentrations were within the range that already guarantee a maximum effect on ductus closure.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Funding: Institut national de la santé et de la recherche médicale (Inserm) is the sponsor of the TREOCAPA trial. The project leading to this application has received funding through the Connect4Children consortium from the Innovative Medicines Initiatives 2 Joint Undertaking under grant agreement n°777389. This joint undertaking receives support from the European Union’s Horizon 2020 research and innovation programme and EFPIA. Role of the funder/sponsor: The funding organisation had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication. Conflict of interest: Faheemah Padavia, Jean-Marc Treluyer, Gilles Cambonie, Cyril Flamant, Aline Rideau, Manon Tauzin, Juliana Patkai, Géraldine Gascoin, Mirka Lumia, Outi Aikio, Frantz Foissac, Saïk Urien, Sihem Benaboud, Gabrielle Lui, Léo Froelicher Bournaud, Yi Zheng, Ruth Kemper, Marine Tortigue, Alban-Elouen Baruteau, Jaana Kallio, Mikko Hallman, Alpha Diallo, Léa Levoyer, Jean-Christophe Roze And Naïm Bouazza declare that they have no potential conflicts of interest that might be relevant to the contents of this manuscript. Ethics approval: The trial was approved by the ethics committee of Centre Hospitalier La Chartreuse (approval number SI 20.03.09.40128) for France and by the regional medical research ethics committee of North Ostrobothnia (approval number 68/06.00.00/20 19) for Finland. Consent to participate: Written informed consent was obtained from both parents of each infant. Consent for publication: Not applicable. Data availability statement: The data that support the findings of this study are available from Institut national de la santé et de la recherche médicale (Inserm) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. However, data are available from the authors upon reasonable request and with permission from Inserm. Author contributions: Concept and design: NB, MH, JMT, JCR. Acquisition of data: GC, CF, AR, MT, JP, GG, ML, OA, YZ, MT, AEB. Analysis and interpretation of data: FP, NB, FF, SU, JCR. Drafting of the manuscript: FP, NB, FF, SU, GL, LFB, JCR. Critical revision of the manuscript for important intellectual content: All authors.
Figures
References
-
- Sivanandan S, Agarwal R. Pharmacological closure of patent ductus arteriosus: selecting the agent and route of administration. Pediatr Drugs. 2016;18:123–38. - PubMed
-
- Gournay V, Savagner C, Thiriez G, Kuster A, Rozé J-C. Pulmonary hypertension after ibuprofen prophylaxis in very preterm infants. Lancet. 2002;359:1486–8. - PubMed
-
- Benitz WE, Committee on Fetus and Newborn, American Academy of Pediatrics. Patent ductus arteriosus in preterm infants. Pediatrics. 2016. 10.1542/peds.2015-3730. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
