

The most effective combination of pharmacological therapy for heart failure with reduced ejection fraction: a network meta-analysis of randomized controlled trials
- PMID: 39578732
- PMCID: PMC11585106
- DOI: 10.1186/s12872-024-04339-3
The most effective combination of pharmacological therapy for heart failure with reduced ejection fraction: a network meta-analysis of randomized controlled trials
Abstract
Background: Evidence for the efficacy of pharmacological therapies for heart failure with reduced ejection fraction (HFrEF) is growing. However, there is no consensus on the most effective treatment for HFrEF. This study aimed to evaluate the most effective combination of pharmacological therapy in patients with HFrEF.
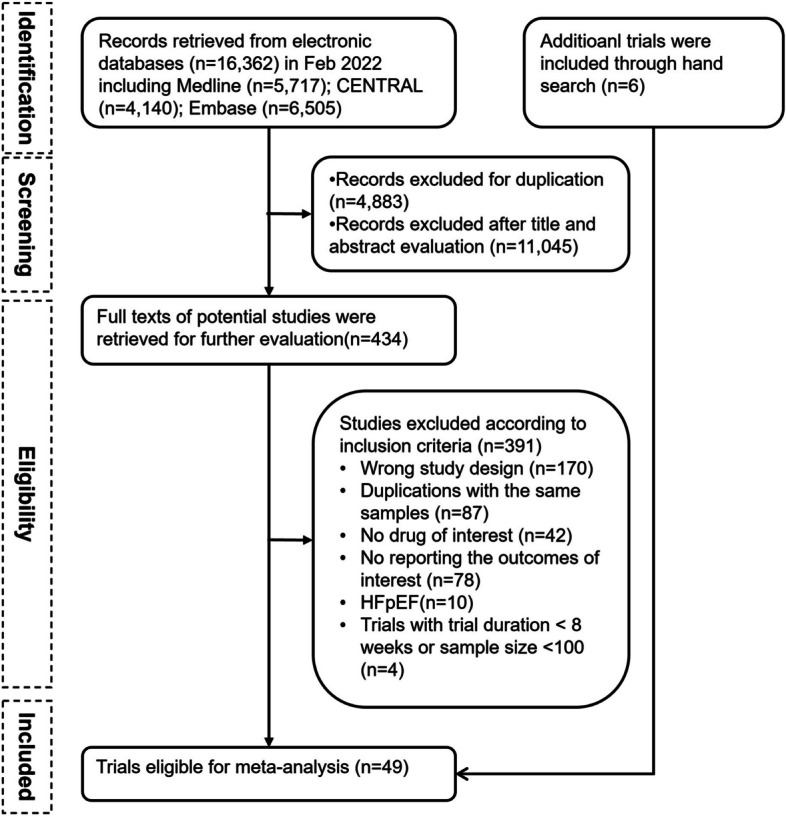
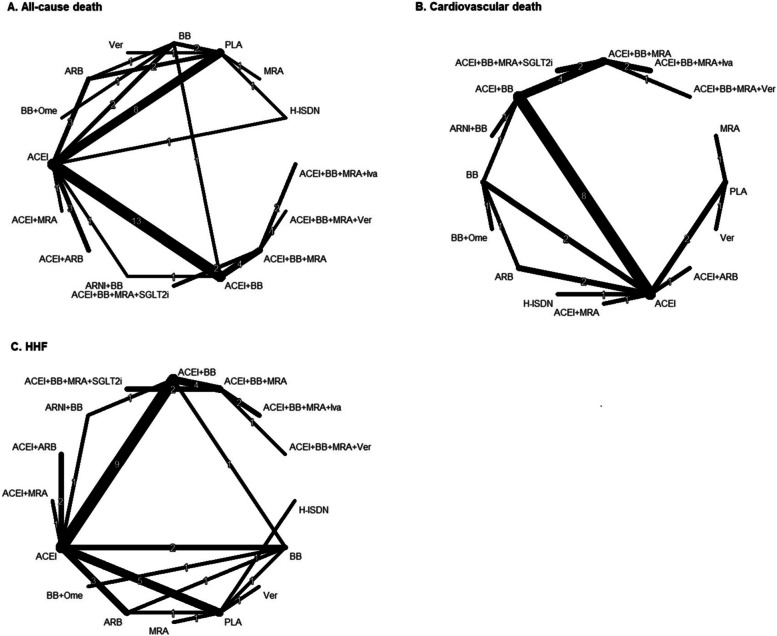
Methods: We systematically searched Medline, Embase, and CENTRAL up to Feb 2022, to include randomized controlled trials (RCTs) that evaluated the efficacy of pharmacological treatment among adults (≥ 18 years) with a diagnosis of HFrEF (defined by a left ventricular ejection fraction ≤ 45%). The outcomes of interest included all-cause death, cardiovascular (CV) death, and hospitalization for heart failure (HHF). A random network meta-analysis using a frequentist framework model was employed to calculate the pooled risk ratio (RR) with 95% confidence interval (CI) and rank the treatments.
Results: We included 49 RCTs involving 90,529 participants with HFrEF. For reducing all-cause mortality, the combination of angiotensin-converting enzyme inhibitors (ACEI), beta-blockers (BB), mineralocorticoid receptor antagonists (MRA), and sodium-glucose co-transporter-2 inhibitors (SGLT2i) was most effective (RR, 0.46; 95% CI, 0.32-0.66). For CV death, the combination of ACEI, BB, MRA, and Vericiguat showed the highest efficacy (RR, 0.34; 95% CI, 0.12-0.90). Regarding reducing HHF, the combination of ACEI, BB, MRA, and SGLT2i as well as the combination of ACEI, BB, MRA, and Ivabradine were equally the most effective (both RR, 0.27; 95% CI, 0.18-0.39).
Conclusion: This study provides robust evidence supporting the use of combination therapies in HFrEF management, with newer agents offering incremental benefits when added to established guideline-directed medical therapy.
Keywords: Heart failure with reduced ejection fraction; Meta-analysis; Pharmacological interventions; Randomized controlled trials.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Murphy SP, Ibrahim NE, Januzzi JL Jr. Heart Failure With Reduced Ejection Fraction: A Review. JAMA. 2020;324(5):488–504. - PubMed
-
- Ponikowski P, Anker SD, AlHabib KF, Cowie MR, Force TL, Hu S, Jaarsma T, Krum H, Rastogi V, Rohde LE, et al. Heart failure: preventing disease and death worldwide. ESC Heart Fail. 2014;1(1):4–25. - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e876–94. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
