

The effects of Dapagliflozin in a real-world population of HFrEF patients with different hemodynamic profiles: worse is better
- PMID: 39578847
- PMCID: PMC11583416
- DOI: 10.1186/s12933-024-02515-5
The effects of Dapagliflozin in a real-world population of HFrEF patients with different hemodynamic profiles: worse is better
Abstract
Background: Sodium-Glucose Cotransporter-2 inhibitors (SGLT2i) represent a deep revolution of the therapeutic approach to heart failure (HF), preventing its insurgence but also improving the management of the disease and slowing its natural progression. To date, few studies have explored the effectiveness of SGLT2i and, in particular, Dapagliflozin in a real-world population. Therefore, in this observational prospective study, we evaluated Dapagliflozin's effectiveness in a real-world HF population categorized in the different hemodynamic profiles.
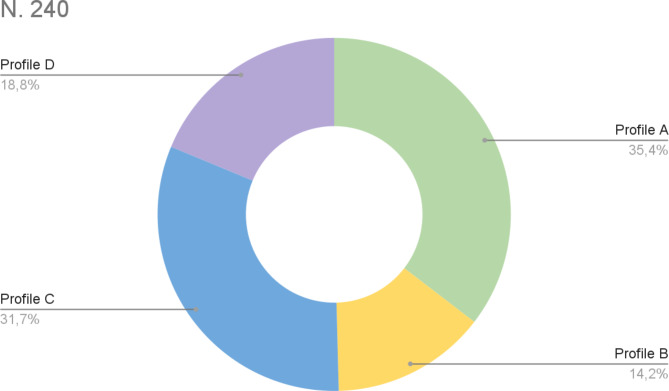
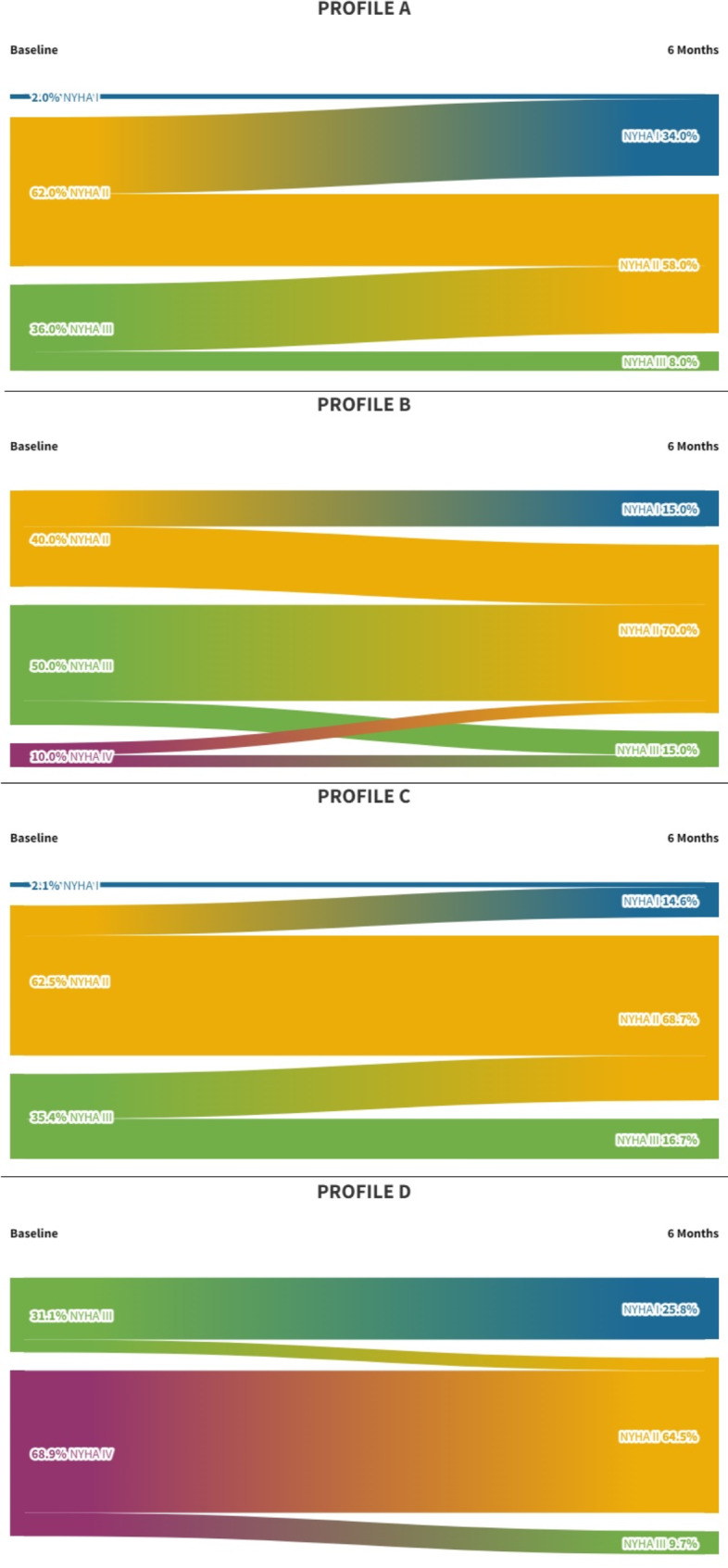
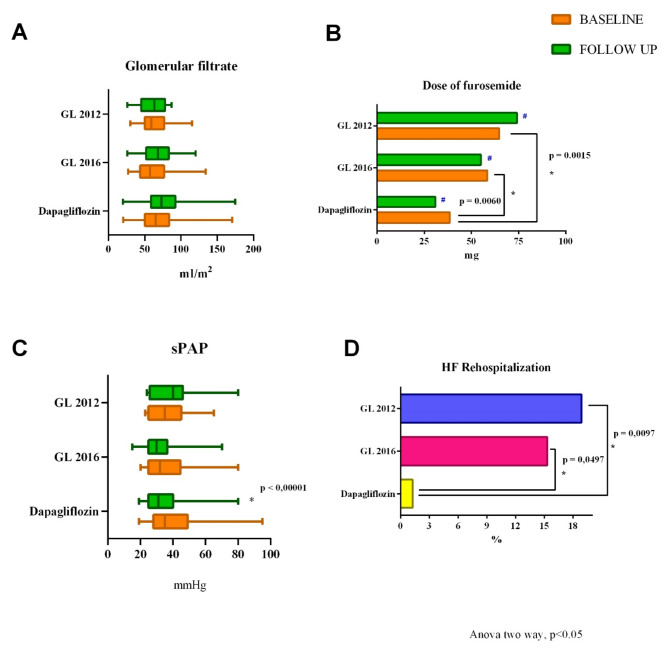
Methods: From January 2022 to June 2023, we enrolled 240 patients with chronic HF and reduced ejection fraction (HFrEF) on optimal medical therapy, according to 2021 ESC guidelines, that added treatment with Dapagliflozin from the HF Clinics of 6 Italian University Hospitals. Clinical, biochemical, and echocardiographic parameters were collected before and after 6 months of Dapagliflozin introduction. Moreover, the HFrEF population was classified according to hemodynamic profiles (A: SV ≥ 35 ml/m2; E/e' < 15; B: SV ≥ 35 ml/m2; E/e' ≥ 15; C: SV < 35 ml/m2; E/e' < 15; D: SV < 35 ml/m2; E/e' ≥ 15). Then, we compared the Dapagliflozin population with two retrospective HF cohorts, hereinafter referred to as Guide Line 2012 (GL 2012) group and Guide Line 2016 (GL 2016) group, in accordance with the HF ESC guidelines in force at the time of patients enrolment. Precisely, we evaluated the changes to baseline in clinical, functional, biochemical, and echocardiographic parameters and compared them to the GL 2012 and GL 2016 groups.
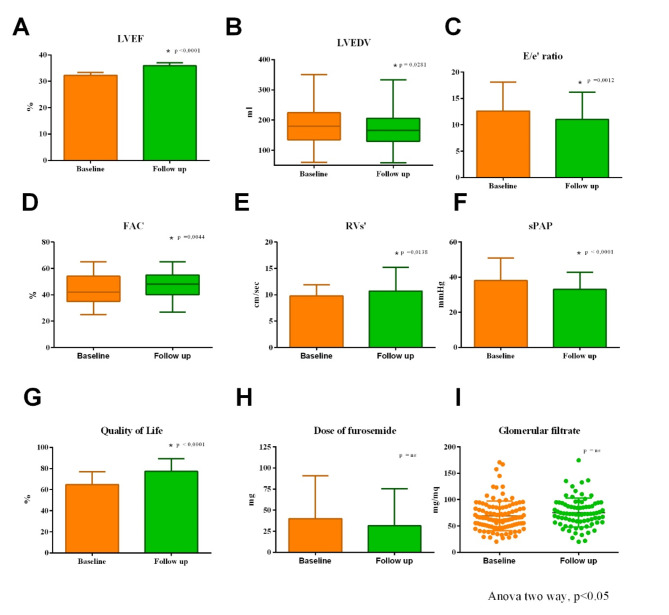
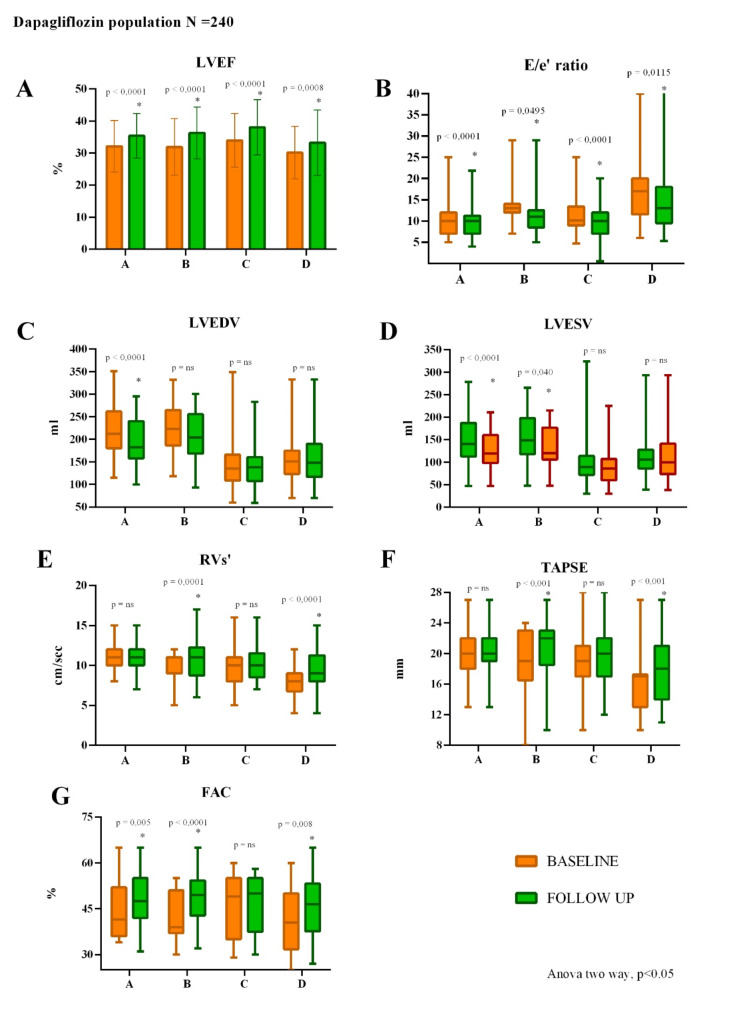
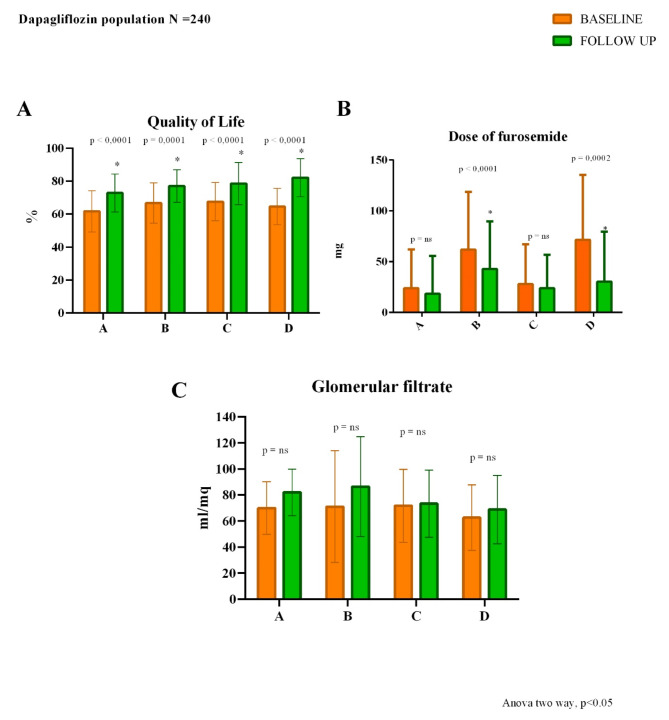
Results: Dapagliflozin population (67.18 ± 11.11 years) showed a significant improvement in the echocardiographic and functional parameters (left ventricular ejection fraction [LVEF], LV end-diastolic volume [LVEDV], LVEDV index, stroke volume index [SVi], left atrium volume index [LAVi], filling pressure [E/e' ratio], tricuspid annular plane systolic excursion [TAPSE], tricuspid annular S' velocity [RVs'], fractional area change [FAC], inferior vena cava [IVC diameter], pulmonary artery systolic pressure [sPAP], NYHA class, and quality of life) compared to baseline. In particular, TAPSE and right ventricle diameter (RVD1) ameliorate in congestive profiles (B and D); accordingly, the furosemide dose significantly decreased in these profiles. Comparing the three populations, the analysis of echocardiographic parameters (baseline vs follow-up) highlighted a significant decrease of sPAP in the Dapagliflozin population (p < 0.05), while no changes were recorded in the GL 2012 and GL 2016 population. Moreover, at the baseline evaluation, the GL 2012 and 2016 groups needed a higher significant dose of furosemide compared to Dapagliflozin group. Finally, Dapagliflozin patients had significantly fewer rehospitalizations (1.25%) compared with the other two groups (GL 2012 18.89%, p 0.0097; GL 2016 15.32%, p 0.0497).
Conclusions: We demonstrate that Dapagliflozin is rapidly effective in an HFrEF real-world population; furthermore, the more significant effect is recorded in HFrEF patients with a congestive profile (B and D), supporting the introduction of Dapagliflozin in patients with a congestive profile and a worse prognosis. In conclusion, our data suggest evaluating the patient's hemodynamic state beyond LVEF in HFrEF.
Keywords: Cardiac function; Dapagliflozin; Heart failure with reduced ejection fraction; Hemodynamic profile; SGLT2 inhibitors.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Informed consent was obtained from all participants. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Visco V, Esposito C, Manzo M, Fiorentino A, Galasso G, Vecchione C, Ciccarelli M. A Multistep Approach to Deal With Advanced Heart Failure: A Case Report on the Positive Effect of Cardiac Contractility Modulation Therapy on Pulmonary Pressure Measured by CardioMEMS. Front Cardiovasc Med. 2022;9: 874433. - DOI - PMC - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e876–94. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
