

Evaluation of severe rhabdomyolysis on day 30 mortality in trauma patients admitted to intensive care: a propensity score analysis of the Traumabase registry
- PMID: 39578880
- PMCID: PMC11585242
- DOI: 10.1186/s13054-024-05158-w
Evaluation of severe rhabdomyolysis on day 30 mortality in trauma patients admitted to intensive care: a propensity score analysis of the Traumabase registry
Abstract
Background: Traumatic rhabdomyolysis (RM) is common and associated with the development of acute kidney injury and potentially with other organ dysfunctions. Thus, RM may increase the risk of death. The primary objective was to assess the effect of severe RM (Creatine Kinase [CK] > 5000 U/L) on 30-day mortality in trauma patients using a causal inference approach.
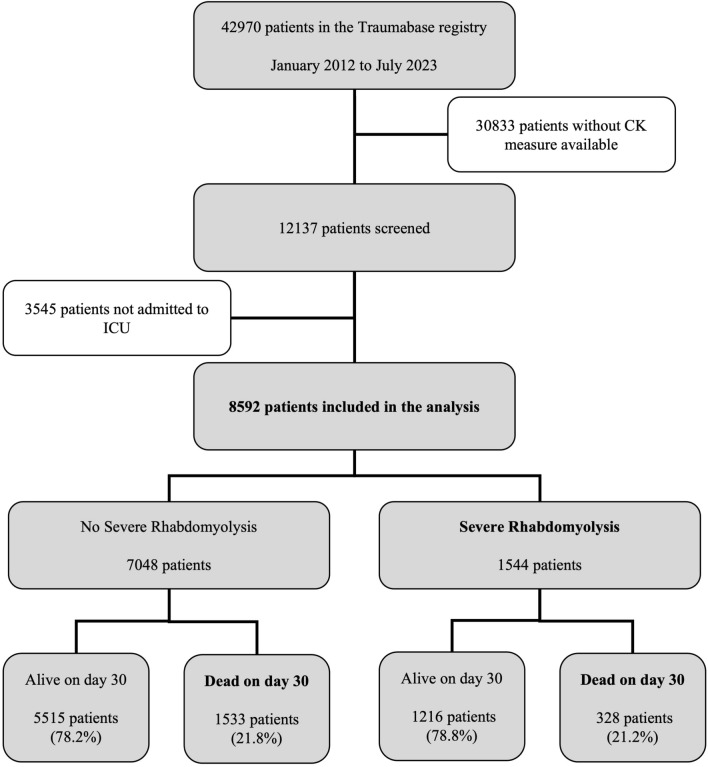
Methods: In this multicenter cohort study conducted in France using a national major trauma registry (Traumabase) between January 1, 2012, and July 1, 2023, all patients admitted to a participating major trauma center hospitalized in intensive care unit (ICU) and with CK measurement were included. Confounding variables for both 30-day mortality and exposure were used to establish a propensity score. A doubly robust approach with inverse treatment weighting enabled the calculation of the average treatment effect on the treated (ATT). Analyses were performed in the overall cohort as well as in two subgroups: hemorrhagic shock subgroup (HS) and traumatic brain injury subgroup (TBI). Sensitivity analyses were conducted.
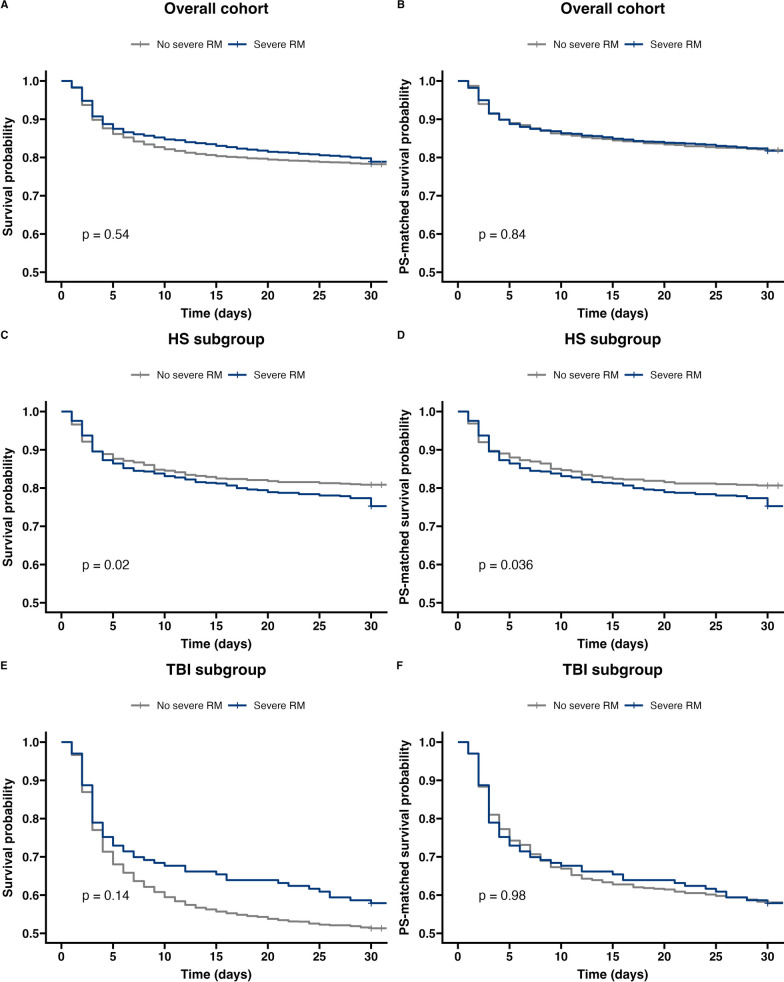
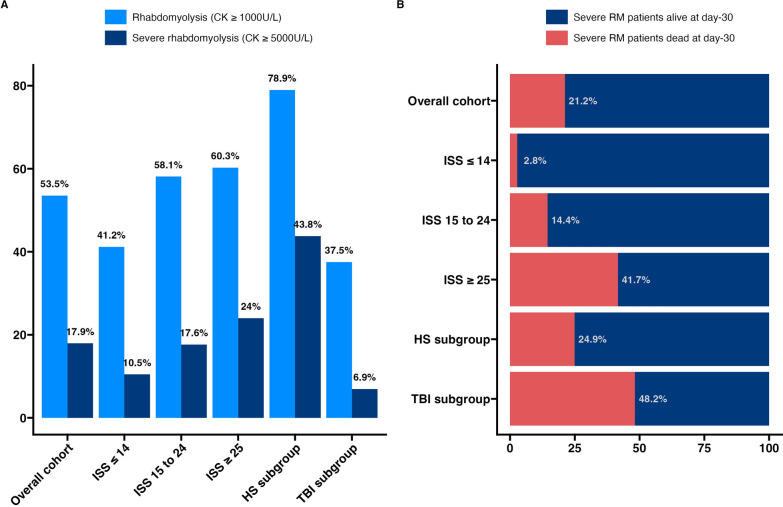
Results: Among the 8592 patients included, 1544 (18.0%) had severe RM. They were predominantly males (78.6%) with median [IQR] age of 41 [27-58] years and severely injured (ISS 20 [13 - 29]) mainly from blunt trauma (90.8%). In the entire cohort, the ATT, expressed as a risk difference, was 0.073 [-0.054 to 0.200]. Considering the 1311 patients in the HS subgroup, the ATT was 0.039 [0.014 to 0.063]. As in the overall cohort, there was no effect on mortality in the TBI subgroup. Severe RM was associated with greater severity of trauma and more complications (whether related to renal function or not) during the ICU stay. Mortality due to multiorgan failure (39.9% vs 12.4%) or septic shock (2.6% vs 0.8%) was more frequent among patients with severe RM.
Conclusions: Severe RM was not associated with 30-day mortality considering the overall cohort. However, it was associated with a 4.0% increase in 30-day mortality among patients with concurrent hemorrhagic shock. Severe RM plays a significant role in ICU morbidity.
Keywords: Crush syndrome; Hemorrhage; Intensive care unit; Multiple organ failure; Rhabdomyolysis; Severe trauma; Trauma related death.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study complies with the STROBE and RECORD (Additional file 4) recommendations for the conduct of retrospective observational studies [41]. It has received the approval of the Paris Nord Research Ethics Committee (IRB number 00006477) and has been declared to the French National Commission on Computing and Liberty (Commission nationale de l’informatique et des libertés, CNIL, N° 2233446). Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
References
-
- Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1736–88. - PMC - PubMed
-
- Eastridge BJ, Holcomb JB, Shackelford S. Outcomes of traumatic hemorrhagic shock and the epidemiology of preventable death from injury. Transfusion. 2019;59(S2):1423–8. - PubMed
-
- Janak JC, Sosnov JA, Bares JM, Stockinger ZT, Montgomery HR, Kotwal RS, et al. Comparison of military and civilian methods for determining potentially preventable deaths: a systematic review. JAMA Surg. 2018;153(4):367. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
