

Evaluation of Risk Factors, and Development and Validation of Prognostic Prediction Models for Distant Metastasis in Patients With Rectal Cancer: A Study Based on the SEER Database and a Chinese Population
- PMID: 39579008
- PMCID: PMC11585045
- DOI: 10.1177/10732748241303650
Evaluation of Risk Factors, and Development and Validation of Prognostic Prediction Models for Distant Metastasis in Patients With Rectal Cancer: A Study Based on the SEER Database and a Chinese Population
Abstract
Purpose: This study aimed to construct a prediction model regarding risk factors and prognostic factors for distant metastasis of T1-T3 stage rectal cancer. For this purpose, a population-based retrospective cohort study was conducted.
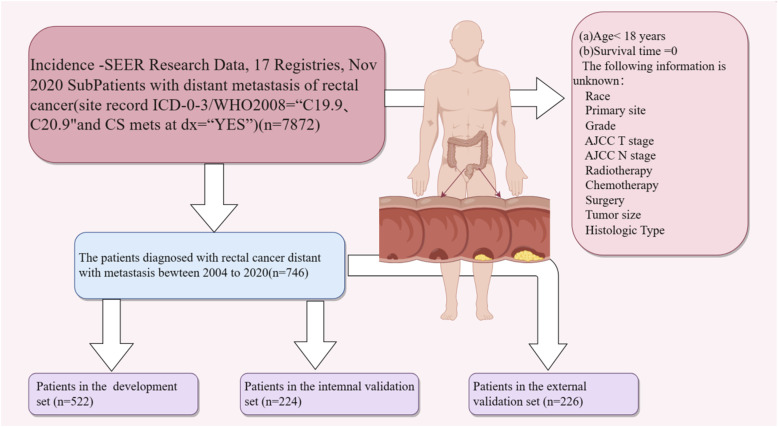
Methods: Data on 7872 patients diagnosed with rectal cancer between 2004 and 2020 were obtained from the Surveillance, Epidemiology, and End Results database, of whom 746 had distant metastases at diagnosis. Independent risk factors for distant metastasis of rectal cancer were determined using univariate and multivariate logistic regression analyses. Cox proportional hazards regression analyses clarified the independent prognostic factors for distant metastases of rectal cancer. A 7:3 randomization process was used to place all patients into the training and internal validation groups. Furthermore, we retrospectively collected clinical data from 226 patients who had both rectal cancer and distant metastases between 2012 and 2024 at the Weifang Hospital of Traditional Chinese Medicine. We used the calibration curve, DCA curve, C-index, and area under the curve (AUC) to assess the discriminatory and pre-precision qualities of the models.
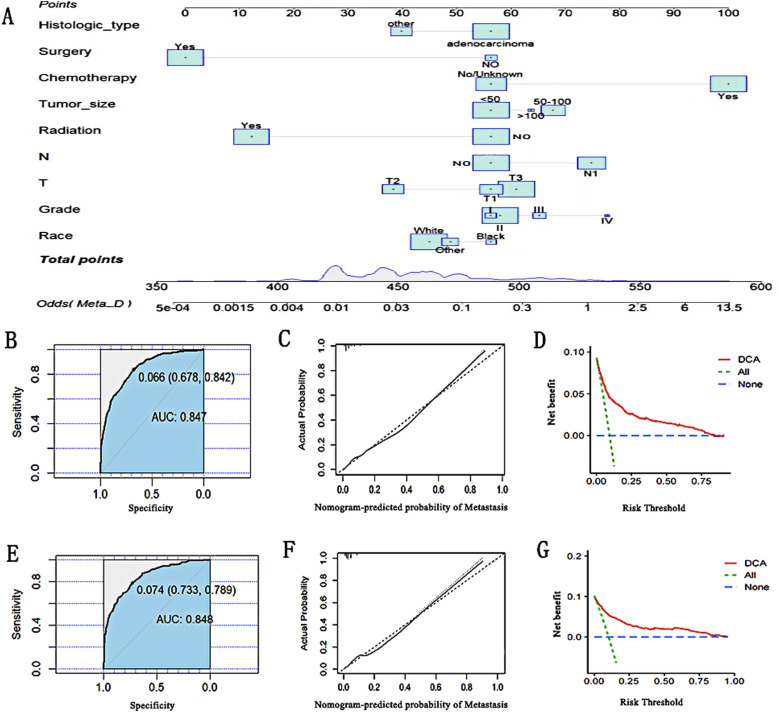
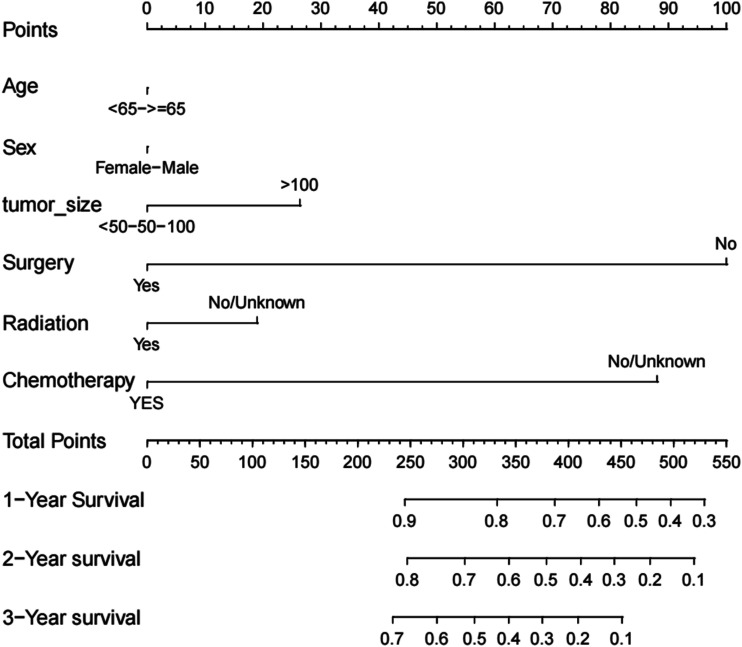
Results: The multivariate logistic regression analysis identified race, tumor grade, T stage, N stage, radiotherapy, chemotherapy, surgery, tumor size, and histological subtype as risk factors for distant metastases in rectal cancer, with AUC values for both training and validation sets exceeding 0.8. Using Cox regression analysis, we determined that the age, sex, tumor size, surgery, chemotherapy, and radiotherapy were independent predictors of distant metastasis of rectal cancer. In the prognostic model, the C-index of the training cohort was 0.687 (95% CI: 0.6615-0.7125), that of the internal validation cohort was 0.692 (95% CI: 0.6508-0.7332), and that of the external validation cohort was 0.704 (0.6785-0.7295).
Conclusion: Our nomogram can predict risk factors and analyze the 1-, 2-, and 3 year prognosis of distant metastases in patients with rectal cancer, providing valuable guidance for future clinical work.
Keywords: distant metastasis; factual database; logistic models; nomogram; prognosis; rectal cancer; risk factors.
Plain language summary
Purpose: This study aimed to construct a prediction model regarding risk factors and prognostic factors for distant metastasis of rectal cancer with T1-T3 stage.
Methods: Data of patients diagnosed with rectal cancer between 2004 and 2020 were obtained from the Surveillance, Epidemiology, and End Results database. Independent risk factors for distant metastasis of rectal cancer were determined using univariate and multivariate logistic regression analyses. Cox proportional risk regression analyses clarified the independent prognostic factors for distant metastases of rectal cancer. A 7:3 randomization process was used to place all patients into the training and internal validation groups. Furthermore, as part of the validation cohort, we retrospectively collected clinical data from 226 patients who had both rectal cancer and distant metastases between 2012 and 2024 at the Weifang Hospital of Traditional Chinese Medicine. We used the calibration curve, DCA curve, C-index, and area under the curve (AUC) to assess the discriminatory and pre-precision qualities of the models.
Results: The multivariate logistic regression analysis revealed that the race, tumor grade, T, N, radiotherapy, chemotherapy, surgery, tumor size, and histological subtype were among the risk factors for distant metastases in rectal cancer, and the AUC values for both the training and validation sets in the risk model were greater than 0.8. Using Cox regression analysis, we determined that the age, sex, tumor size, surgery, chemotherapy, and radiotherapy were independent predictors of distant metastasis of rectal cancer. In the prognostic model, the C-index of the training cohort was 0.687 (95% CI: 0.6615-0.7125), that of the internal validation cohort was 0.692 (95% CI: 0.6508-0.7332), and that of the external validation cohort was 0.704 (0.6785-0.7295).
Conclusion: Our nomogram can predict risk factors and analyze the 1-, 2-, and 3 year prognosis of patients with metastatic rectal cancer, providing valuable guidance for future clinical work.
Conflict of interest statement
Declaration of Conflicting InterestThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Constructing a prognostic model for colorectal cancer with synchronous liver metastases after preoperative chemotherapy: a study based on SEER and an external validation cohort.Clin Transl Oncol. 2024 Dec;26(12):3169-3190. doi: 10.1007/s12094-024-03513-5. Epub 2024 Jun 4. Clin Transl Oncol. 2024. PMID: 38834909 Free PMC article.
-
Development and validation of predictive models for distant metastasis and prognosis of gastroenteropancreatic neuroendocrine neoplasms.Sci Rep. 2025 Mar 19;15(1):9510. doi: 10.1038/s41598-025-92974-x. Sci Rep. 2025. PMID: 40108260 Free PMC article.
-
Nomogram predicting overall survival of rectal squamous cell carcinomas patients based on the SEER database: A population-based STROBE cohort study.Medicine (Baltimore). 2019 Nov;98(46):e17916. doi: 10.1097/MD.0000000000017916. Medicine (Baltimore). 2019. PMID: 31725640 Free PMC article.
-
A New Online Dynamic Nomogram: Construction and Validation of a Predictive Model for Distant Metastasis Risk and Prognosis in Patients with Gastrointestinal Stromal Tumors.J Gastrointest Surg. 2023 Jul;27(7):1429-1444. doi: 10.1007/s11605-023-05706-9. Epub 2023 May 25. J Gastrointest Surg. 2023. PMID: 37231240 Review.
-
A nomogram for predicting the risk of liver metastasis in non-functional neuroendocrine neoplasms: A population-based study.Eur J Surg Oncol. 2025 May;51(5):109708. doi: 10.1016/j.ejso.2025.109708. Epub 2025 Feb 21. Eur J Surg Oncol. 2025. PMID: 40024114 Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
