

Determinants of non-adherence to antibiotic treatment guidelines in hospitalized adults with suspected community-acquired pneumonia: a prospective study
- PMID: 39580437
- PMCID: PMC11585212
- DOI: 10.1186/s13756-024-01494-2
Determinants of non-adherence to antibiotic treatment guidelines in hospitalized adults with suspected community-acquired pneumonia: a prospective study
Abstract
Background: Antimicrobial resistance (AMR) is a global health threat with millions of deaths annually attributable to bacterial resistance. Effective antimicrobial stewardship programs are crucial for optimizing antibiotic use. This study aims to identify factors contributing to deviations from antibiotic treatment guidelines in hospitalized adults with suspected community-acquired pneumonia (CAP).
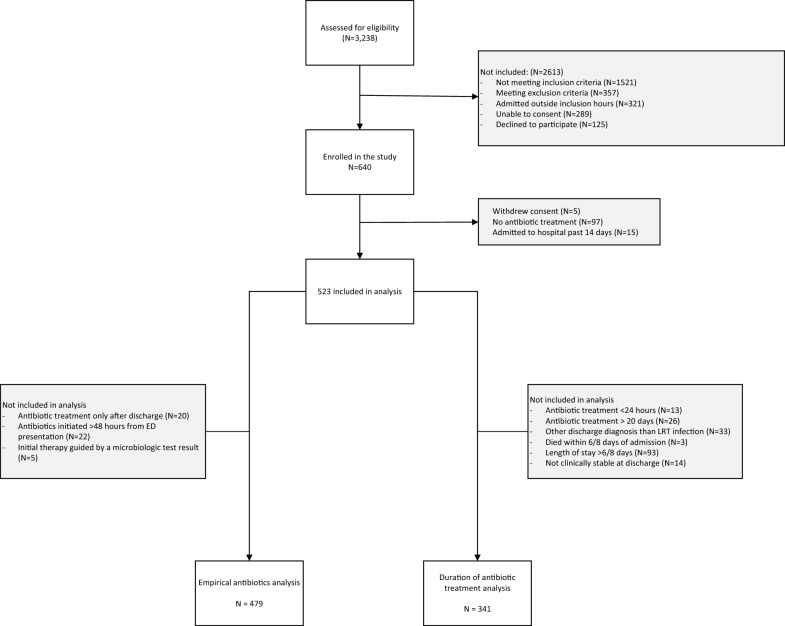
Methods: We conducted a prospective study at Haukeland University Hospital's Emergency Department in Bergen, Norway, from September 2020 to April 2023. Patients were selected from two cohorts, with data on clinical and microbiologic test results collected. We analysed adherence of antibiotic therapy to guidelines for the choice of empirical treatment and therapy duration using multivariate regression models to identify predictors of non-adherence.
Results: Of the 523 patients studied, 479 (91.6%) received empirical antibiotic therapy within 48 h of admission, with 382 (79.7%) adhering to guidelines. However, among the 341 patients included in the analysis of treatment duration adherence, only 69 (20.2%) received therapy durations that were consistent with guideline recommendations. Key predictors of longer-than-recommended therapy duration included a C-reactive protein (CRP) level exceeding 100 mg/L (RR 1.37, 95% CI 1.18-1.59) and a hospital stay longer than two days (RR 1.22, 95% CI 1.04-1.43). The primary factor contributing to extended antibiotic therapy duration was planned post-discharge treatment. No significant temporal trends in adherence to treatment duration guidelines were observed following the publication of the updated guidelines.
Conclusion: While adherence to guidelines for the choice of empirical antibiotic therapy was relatively high, adherence to guidelines for therapy duration was significantly lower, largely due to extended post-discharge antibiotic treatment. Our findings suggest that publishing updated guidelines alone is insufficient to change clinical practice. Targeted stewardship interventions, particularly those addressing discharge practices, are essential. Future research should compare adherence rates across institutions to identify factors contributing to higher adherence and develop standardized benchmarks for optimal antibiotic stewardship. Trial registration NCT04660084.
Keywords: Antibiotic stewardship; Antibiotic therapy duration; Antimicrobial resistance (AMR); C-reactive protein (CRP); COPD; Community-acquired pneumonia (CAP); Empirical antibiotic therapy; Guideline adherence; Hospital discharge practices.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study is approved by the Regional Committee for Medical and Health Research Ethics in South East Norway (REK ID: 31935) and performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants or their legal guardian/close relative at the time of recruitment. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Hijazi K, Joshi C, Gould IM. Challenges and opportunities for antimicrobial stewardship in resource-rich and resource-limited countries. Expert Rev Anti Infect Ther. 2019;17(8):621–34. - PubMed
-
- Harris AM, Hicks LA, Qaseem A. Appropriate antibiotic use for acute respiratory tract infection in adults: advice for high-value care from the American college of physicians and the centers for disease control and prevention. Ann Intern Med. 2016;164(6):425–34. - PubMed
-
- Peyrani P, Mandell L, Torres A, Tillotson GS. The burden of community-acquired bacterial pneumonia in the era of antibiotic resistance. Expert Rev Respir Med. 2019;13(2):139–52. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
