

Hyporesponsiveness to Erythropoiesis-Stimulating Agents in Dialysis-Dependent Patients with Anaemia of Chronic Kidney Disease: A Retrospective Observational Study
- PMID: 39581908
- PMCID: PMC11782378
- DOI: 10.1007/s12325-024-03015-4
Hyporesponsiveness to Erythropoiesis-Stimulating Agents in Dialysis-Dependent Patients with Anaemia of Chronic Kidney Disease: A Retrospective Observational Study
Abstract
Introduction: Hyporesponsiveness to erythropoiesis-stimulating agents (ESAs) in patients with anaemia of chronic kidney disease may lead to increased ESA doses to achieve target haemoglobin levels; however, elevated doses may be associated with increased mortality. Furthermore, patients with hyporesponsiveness to ESAs have poorer clinical outcomes than those who respond well to ESAs. Incidence and clinical characteristics of patients with ESA hyporesponsiveness were explored in a real-world setting.
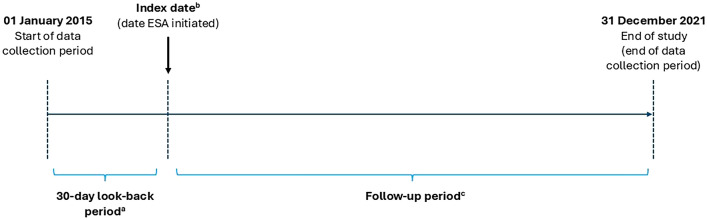
Methods: This was a retrospective study of electronic medical records of adults with stage 5 chronic kidney disease receiving renal replacement therapy and ESA treatment, from 1 January 2015 to 31 December 2021. The primary objective was ESA hyporesponsiveness rate/1000 days, with a hyporesponsive event defined as ESA use at an elevated dose, according to National Institute for Health and Care Excellence (NICE) criteria. Other hyporesponsiveness definitions applied were erythropoietin resistance index-defined ESA hyporesponsiveness (ERI) Kidney Disease Improving Global Outcomes (KDIGO) and a clinical practicality algorithm.
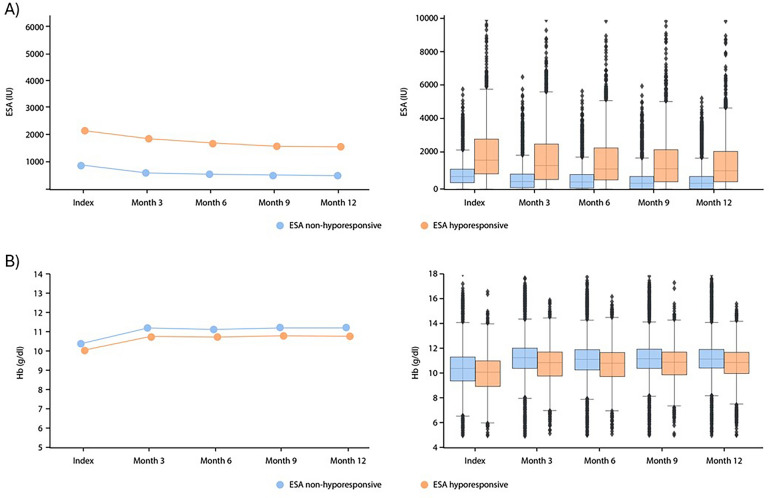
Results: In total, 85,259 patients were included in the analysis; 59.9% were male, median (interquartile range) ESA starting dose was 733.3 (400.0, 1200.0) IU/week and follow-up duration was 2.2 (1.0, 4.2) years. Incidence of ESA hyporesponsiveness varied when applying different definitions; NICE 0.05/1000 days (5.2% of patients), ERI 0.40/1000 days (40.7%), KDIGO 0.15/1000 days (15.4%), and clinical practicality algorithm 0.48/1000 days (47.9%). ESA doses remained higher in hyporesponsive versus responsive patients, yet haemoglobin levels were similar between groups.
Conclusion: The results from this study, which applied multiple hyporesponsiveness definitions to a large, geographically diverse population of patients with anaemia of CKD, showed variation in ESA hyporesponsiveness incidence rates depending on definitions used and higher ESA doses in hyporesponsive versus responsive patients. These results underscore the need for individualised clinical assessment and thorough evaluation when considering ESA dose adjustments to reach haemoglobin targets. Graphical abstract available for this article.
Trial registration: NCT05530291.
Keywords: Anaemia; CKD; Dialysis; Erythropoiesis-stimulating agent; Hyporesponsiveness.
Plain language summary
Some people living with kidney disease may also have anaemia (low numbers of blood cells). This can increase their risk of heart disease and reduce their quality of life. Treatments for anaemia in people living with kidney disease include iron supplements and drugs that stimulate the production of red blood cells, known as erythropoiesis-stimulating agents. However, some people have weak responses to erythropoiesis-stimulating agents, and high doses can cause side effects. We looked at how the percentage of people with weak responses to erythropoiesis-stimulating agents varied when using different criteria to identify them. We also looked at the clinical characteristics of people who experienced a weak response after 1 year and those who did not. To do this, we reviewed medical records from people treated at specialist kidney care centres across 24 countries from Europe and South Africa. We included medical records between 1 January 2015 and 31 December 2021. Depending on what criteria we used, the percentage of people living with kidney disease and anaemia who were identified as having weak responses to erythropoiesis-stimulating agents varied greatly, from 5.2% to 47.9%. People living with kidney disease and anaemia who have weak responses to treatment with erythropoiesis-stimulating agents need adjustments to their care to address this. However, our research shows that the different criteria used to identify these patients can affect how many are identified, and may affect their care. Therefore, all patients with kidney disease and anaemia should be carefully monitored.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: Hans-Jürgen Aren, Luca Neri, Astrid Feuersenger, Mario Garbelli and Otto Arkossy are employees of Fresenius Medical Care, contracted by Astellas Pharma Global Development Inc. to conduct the study. Hans-Jürgen Aren reports Fresenius Medical Care stock shares. Christopher Atzinger and Alina Jiletcovici are employees of Astellas Pharma Global Development Inc. Alina Jiletcovici reports Eli Lilly stock shares. Robert Snijder is an employee of Astellas Pharma Europe B.V. Kirsten Leyland, Najib Khalife and Mahmood Ali are employees of Astellas Pharma Europe Ltd. Ethical Approval: All data were pseudonymised and all patients provided written informed consent for access and secondary use of their pseudonymised clinical data for research purposes. According to the National Institutes of Health definition of human subject research, this study falls under the exempt human subjects research category [27].
Figures
References
-
- Institute for Health Metrics and Evaluation. Chronic Kidney Disease – Level 3 cause. 2022. https://www.healthdata.org/results/gbd_summaries/2019/chronic-kidney-dis.... Accessed 2023 Dec 15.
-
- Nakhoul G, Simon JF. Anemia of chronic kidney disease: treat it, but not too aggressively. Cleve Clin J Med. 2016;83(8):613–24. 10.3949/ccjm.83a.15065. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
