

Pharmacokinetics of Omadacycline in Adults with Cystic Fibrosis
- PMID: 39581957
- PMCID: PMC11649715
- DOI: 10.1007/s40262-024-01440-w
Pharmacokinetics of Omadacycline in Adults with Cystic Fibrosis
Abstract
Background: Omadacycline offers a potential advancement in the management of infections in people with cystic fibrosis (CF) because of its spectrum of activity, intrapulmonary penetration, and oral bioavailability. A prospective single-dose, single-arm study was conducted to characterize the pharmacokinetic (PK) profile of omadacycline in people with CF, considering the known alterations in PK observed in this population (NCT04460586, 2020-07-01).
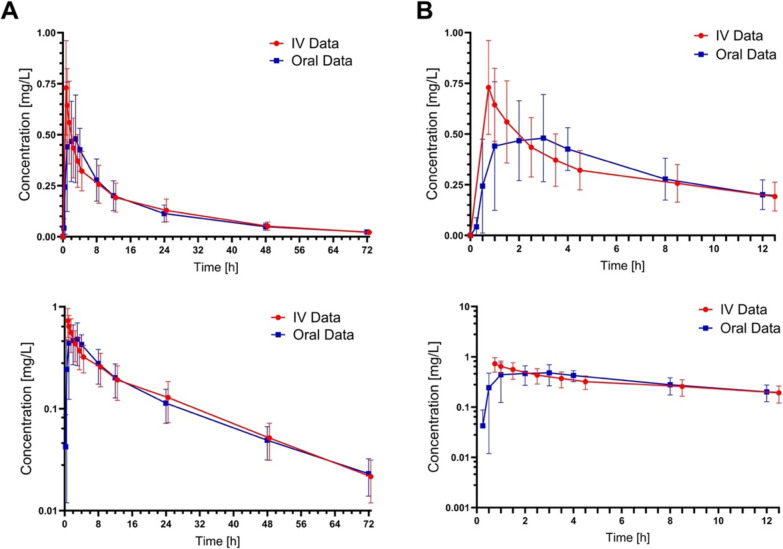
Methods: Plasma samples were obtained from nine adults with CF who received a single dose of intravenous omadacycline 100 mg over 0.5 h followed by a 1-week washout and an oral dose of omadacycline 300 mg. The data were analyzed using noncompartmental PK.
Results: The maximum plasma concentration (Cmax) and area under the curve extrapolated to infinity (AUC0-∞) after intravenous administration of omadacycline were similar between healthy volunteers and people with CF. The absorption kinetics of oral omadacycline, encompassing both the rate (Cmax and time to Cmax [tmax]) and the extent (AUC0-∞), also showed consistency between healthy volunteers and people with CF. The absolute bioavailability of the oral tablet formulation of omadacycline in people with CF (31.2%) was also consistent with that observed in healthy volunteers (34.5%). In comparing the two routes of administration, intravenous omadacycline 100 mg provided plasma exposures equivalent to those with oral omadacycline 300 mg in people with CF, as evidenced by geometric mean ratios for both AUC0-∞ (0.9381; 90% confidence intervals [CI] 0.6783-1.2975) and Cmax (0.7746; 90% CI 0.5478-1.0951).
Conclusions: Overall, the similarity in plasma PK observed in this study when comparing healthy volunteers and infected patients indicates that no dosing alterations are necessary when using omadacycline in people with CF.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Funding: Open access funding provided by SCELC, Statewide California Electronic Library Consortium. This study was supported by Paratek Pharmaceuticals, Inc. as an investigator-initiated grant. Conflicts of Interest: The authors have no conflicts of interest to declare. Ethics Approval: The study protocol was approved by the University of Southern California institutional review board (HS-20-00513), and the study was conducted in compliance with the ethical standards established in the 1964 Declaration of Helsinki and its subsequent amendments. Consent for publication: Written informed consent for publication of identifiable details, including clinical data, was obtained from the patient (or their legal guardian) prior to submission of this manuscript, in accordance with Adis Publishing ethical guidelines. Consent to Participate: All participants provided written informed consent before the study. Availability of Data and Material: The data that support the findings of this study are available from the corresponding author upon reasonable request. Data sharing will be subjected to standard data use agreements from the University of Southern California. Author Contributions: All authors contributed to the study conception and design. Data were collected by Peter Chung and Adupa Rao. Data were analyzed by Eunjin Hong, Madeline Sanders, and Paul Beringer. The first draft of the manuscript was written by Madeline Sanders, and all authors commented on subsequent versions of the manuscript. All authors read and approved the final manuscript.
Figures

References
-
- Adjemian J, Olivier KN, Prevots DR. Epidemiology of pulmonary nontuberculous mycobacterial sputum positivity in patients with cystic fibrosis in the United States, 2010–2014. Ann Am Thorac Soc. 2018;15(7):817–26. 10.1513/AnnalsATS.201709-727OC. (Erratum in: Ann Am Thorac Soc. 2018;15(9):1114–5). - PMC - PubMed
-
- Bernut A, Dupont C, Ogryzko NV, et al. CFTR protects against Mycobacterium abscessus infection by fine-tuning host oxidative defenses. Cell Rep. 2019;26(7):1828-40.e4. 10.1016/j.celrep.2019.01.071. - PubMed
-
- Barto TL, Olivier KN. Nontuberculous mycobacteria clinical care guidelines. Cystic Fibrosis Foundation. 2016. https://www.cff.org/medical-professionals/nontuberculous-mycobacteria-cl...
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
