

Oxygenation indices and early prediction of outcome in hypoxemic patients with COVID-19 pneumonia requiring noninvasive respiratory support in pulmonary intermediate care unit
- PMID: 39582005
- PMCID: PMC11587655
- DOI: 10.1186/s41479-024-00145-9
Oxygenation indices and early prediction of outcome in hypoxemic patients with COVID-19 pneumonia requiring noninvasive respiratory support in pulmonary intermediate care unit
Abstract
Background: Early prediction of non-invasive respiratory therapy (NIRT) failure is crucial to avoid needless prolongation of respiratory support and delayed endotracheal intubation. Data comparing the predictive value of oxygenation indices (OI) in COVID-19 receiving NIRT are scant. The aim of this monocentric retrospective study of prospectively collected data was to assess the effectiveness of different OI in predicting NIRT outcome at baseline (t0), 12 h (t12) and 24 h (t24) of treatment in hypoxemic patients with COVID-19-related pneumonia, managed in a Pulmonary Intermediate Care Unit (October 2020-June 2021).
Methods: We assessed the predictive value of SpO2/FiO2, PaO2/FiO2, standardised PaO2/FiO2 ratio (s-PaO2/FiO2), respiratory index (RI), arterial-alveolar oxygen gradient (a-ADO2), age adjusted arterial-alveolar oxygen ratio (adj-a-ADO2D). Receiver operating characteristics (ROC), AUC and best sensitivity-specificity cut-off values were calculated at t0, t12, t24. NIRT failure risk was adjusted for non-oxygenation predictors.
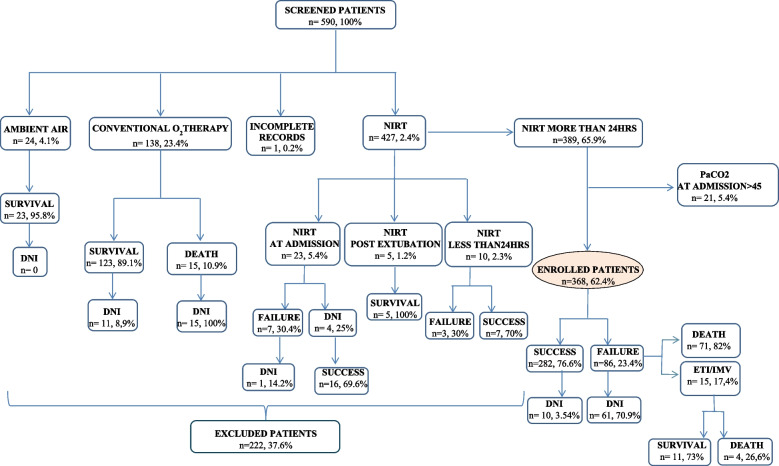
Results: Among 590 patients with COVID-19 infection, 368 met the eligibility criteria for inclusion in the study [mean (CI95%): PaO2/FiO2 214(206,8-221,9); PaCO2 mean 32,9 mmHg,(32,4-33,4)]. NIRT failure and hospital mortality rate were 23,4% and 19,6%, respectively. Older age, male gender, agitation/confusion, need for sedation, inability to tolerate prone positioning were independent predictors of NIRT failure. SpO2/FiO2, a-ADO2 and adj-aADO2 at t12 and t24, PaO2/FiO2 and RI at t24 were associated with NIRT failure. Prognostic predictivity of OI increased from t0 to t24. Greater ROC-AUC values were obtained with SpO2/FiO2 0,662 (0,60-0,72) (t0), PaO2/FiO2 0,697 (0,63-0,76) (t12) and s-PaO2/FiO2 0,769 (0,71-0,83) (t24). NIRT failure was independently predicted by PaO2/FiO2, s-PaO2/FiO2 and RI at any observation time and by SpO2/FiO2 and O2 gradients respectively at t0 and t24. SaO2/FiO2 ≤ 300 (t0), PaO2/FiO2 ≤ 151,7 (t12) and s-PaO2/FiO2 ≤ 160,4 (t24) turned out to be the best predictors of NIRT outcome.
Conclusions: OI showed different effectiveness in predicting NIRT failure within 24 h of treatment in COVID-19 related pneumonia. This may be due to the multi-factorial pathophysiology of hypoxemia. Our study empathises furthermore the role of non-oxygenation-related parameters in contributing to the outcome. These findings may be useful to build a predictive model also in no COVID-19 related hypoxemic pneumonia.
Keywords: COVID-19; High flow nasal cannula; Non invasive respiratory therapies; Non invasive ventilation; Oxygenation indexes; Pulmonary intermediate care unit.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: -Ethical Committee’s approval and a written informed patient consent were achieved. -The name of Ethical Committee is referred to Usl Toscana Sudest, Arezzo, Italy. -Ethical issues for any animal data or tissue: NA. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
Correlation and Prognostic Significance of Oxygenation Indices in Invasively Ventilated Adults (OXIVA-CARDS) with COVID-19-associated ARDS: A Retrospective Study.Indian J Crit Care Med. 2023 Nov;27(11):801-805. doi: 10.5005/jp-journals-10071-24560. Indian J Crit Care Med. 2023. PMID: 37936792 Free PMC article.
-
[Comparison of pulse oxygen saturation/fraction of inhaled oxygen and arterial partial pressure of oxygen/fraction of inhaled oxygen in the assessment of oxygenation in acute respiratory distress syndrome patients at different high altitudes in Yunnan Province].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 Jul;33(7):826-831. doi: 10.3760/cma.j.cn121430-20210301-00303. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 34412752 Chinese.
-
[Efficacy of high flow nasal oxygen therapy in children with acute respiratory failure].Zhonghua Er Ke Za Zhi. 2021 Jan 2;59(1):20-26. doi: 10.3760/cma.j.cn112140-20200612-00617. Zhonghua Er Ke Za Zhi. 2021. PMID: 33396999 Chinese.
-
Oxygen therapy and noninvasive respiratory supports in acute hypoxemic respiratory failure: a narrative review.Ann Intensive Care. 2024 Oct 18;14(1):158. doi: 10.1186/s13613-024-01389-w. Ann Intensive Care. 2024. PMID: 39419924 Free PMC article. Review.
-
Non-invasive ventilatory support and high-flow nasal oxygen as first-line treatment of acute hypoxemic respiratory failure and ARDS.Intensive Care Med. 2021 Aug;47(8):851-866. doi: 10.1007/s00134-021-06459-2. Epub 2021 Jul 7. Intensive Care Med. 2021. PMID: 34232336 Free PMC article. Review.
Cited by
-
Intrapulmonary and intrabronchial oxygen-producing antihypoxants eliminate asphyxia and hypoxemia.Med Gas Res. 2025 Dec 1;15(4):550-551. doi: 10.4103/mgr.MEDGASRES-D-25-00027. Epub 2025 Apr 29. Med Gas Res. 2025. PMID: 40300893 Free PMC article. No abstract available.
References
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239–42. 10.1001/JAMA.2020.2648. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
