

Stress hyperglycemia ratio association with all-cause mortality in critically ill patients with coronary heart disease: an analysis of the MIMIC-IV database
- PMID: 39582018
- PMCID: PMC11586423
- DOI: 10.1038/s41598-024-80763-x
Stress hyperglycemia ratio association with all-cause mortality in critically ill patients with coronary heart disease: an analysis of the MIMIC-IV database
Abstract
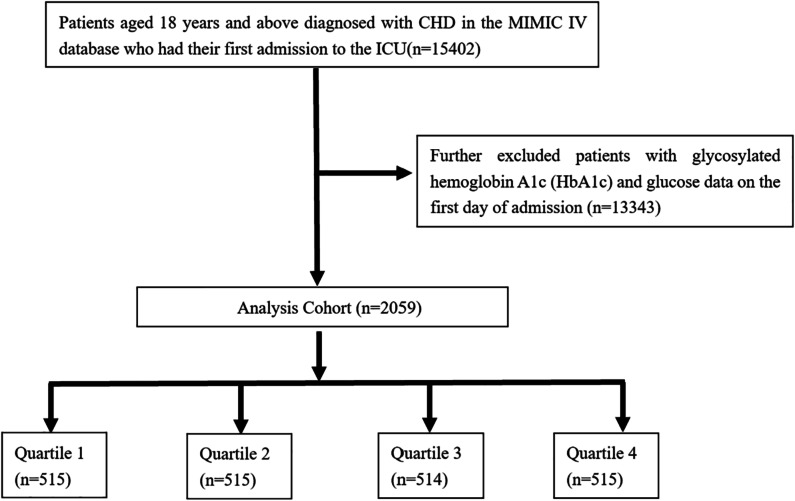
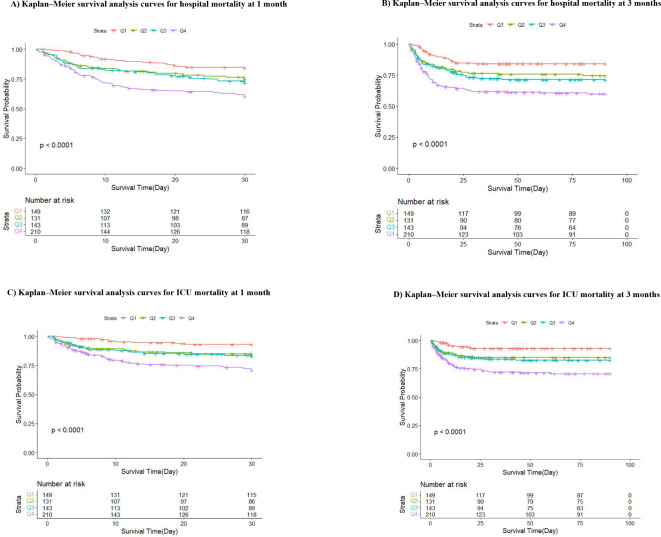
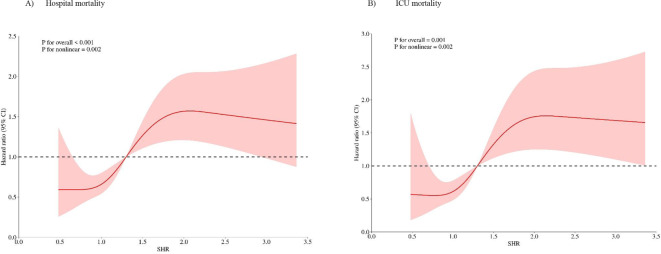
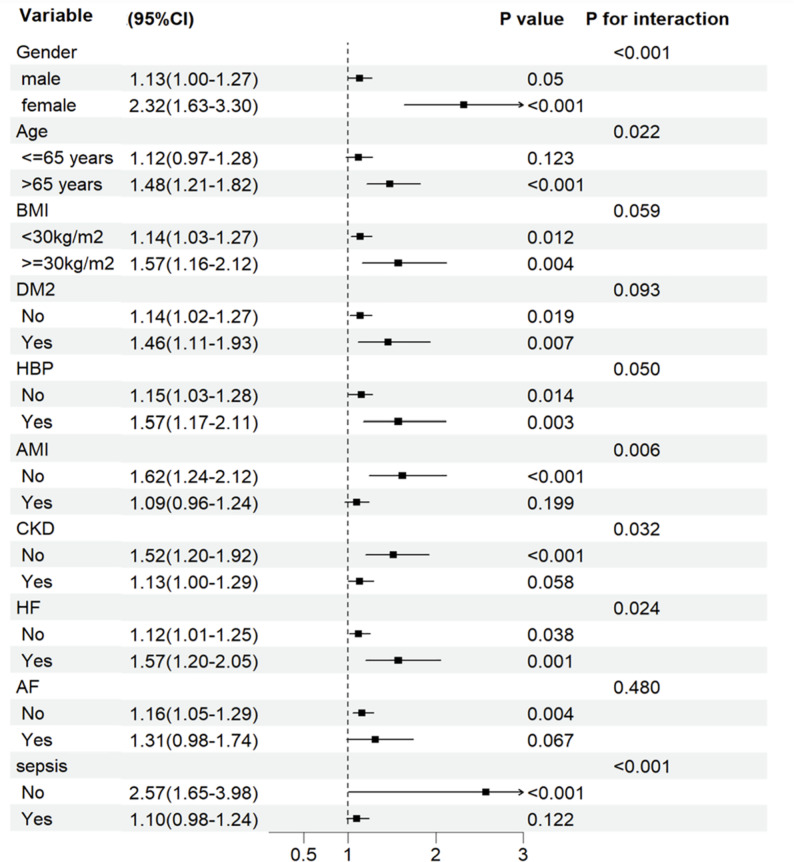
Background The stress hyperglycemia ratio (SHR) indicates relative hyperglycemia levels. Research on the impact of SHR on mortality in coronary heart disease (CHD) patients in intensive care is limited. This study explores the predictive accuracy of SHR for the prognosis of CHD patients in the ICU. Methods This study included 2,059 CHD patients from the American Medical Information Mart for Intensive Care (MIMIC-IV) database. SHR was determined using the formula: SHR = (admission glucose) (mmol/L) / (1.59 * HbA1c [%] - 2.59). Subjects were stratified into quartiles based on SHR levels to examine the correlation between SHR and in-hospital mortality. The restricted cubic splines and Cox proportional hazards models were employed to assess this association, while Kaplan-Meier survival analysis was executed to ascertain the mortality rates across the SHR quartiles. Results Among the 2059 participants (1358 men), the rates of in-hospital and ICU mortality were 8.5% and 5.25%, respectively. Analysis showed SHR as a significant predictor of increased risk for both in-hospital (HR,1.16, 95% CI: 1.02-1.32, P = 0.022) and ICU mortality (HR, 1.16, 95% CI: 1.01-1.35, P = 0.040) after adjustments. A J-shaped relationship was noted between SHR and mortality risks (p for non-linearity = 0.002, respectively). Kaplan-Meier analysis confirmed substantial differences in in-hospital and ICU mortality across SHR quartiles. Conclusions SHR significantly predicts in-hospital and ICU mortality in critically ill CHD patients, indicating that higher SHR levels correlate with longer ICU stays and increased mortality. This underscores the potential of SHR as a prognostic marker for ICU CHD patients.
Keywords: Coronary heart disease; MIMIC-IV database; Mortality; Stress hyperglycemia ratio.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval: Not applicable.
Figures
Similar articles
-
Association between stress hyperglycemia ratio index and all-cause mortality in critically ill patients with atrial fibrillation: a retrospective study using the MIMIC-IV database.Cardiovasc Diabetol. 2024 Oct 14;23(1):363. doi: 10.1186/s12933-024-02462-1. Cardiovasc Diabetol. 2024. PMID: 39402588 Free PMC article.
-
Unveiling the role of stress hyperglycemia in predicting mortality for critically ill hemorrhagic stroke patients: insights from MIMIC-IV.Front Endocrinol (Lausanne). 2025 May 2;16:1558352. doi: 10.3389/fendo.2025.1558352. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40385356 Free PMC article.
-
Stress hyperglycemia ratio linked to all-cause mortality in critically ill patients with ischemic heart disease.BMC Cardiovasc Disord. 2025 May 19;25(1):374. doi: 10.1186/s12872-025-04831-4. BMC Cardiovasc Disord. 2025. PMID: 40389863 Free PMC article.
-
Stress hyperglycemia ratio as a mortality predictor in non-diabetic septic patients: a retrospective cohort analysis.BMC Infect Dis. 2025 May 25;25(1):752. doi: 10.1186/s12879-025-11151-7. BMC Infect Dis. 2025. PMID: 40414847 Free PMC article.
-
The prognostic value of the stress hyperglycemia ratio for all-cause mortality in stroke patients with diabetes or prediabetes.J Diabetes Complications. 2025 Apr;39(4):108979. doi: 10.1016/j.jdiacomp.2025.108979. Epub 2025 Mar 5. J Diabetes Complications. 2025. PMID: 40090129
Cited by
-
Association between stress hyperglycemia ratio and neovascular glaucoma in patients with proliferative diabetic retinopathy.BMC Ophthalmol. 2025 Apr 1;25(1):163. doi: 10.1186/s12886-025-03982-4. BMC Ophthalmol. 2025. PMID: 40170000 Free PMC article.
-
The prognostic significance of stress hyperglycemia ratio in evaluating all-cause and cardiovascular mortality risk among individuals across stages 0-3 of cardiovascular-kidney-metabolic syndrome: evidence from two cohort studies.Cardiovasc Diabetol. 2025 Mar 24;24(1):137. doi: 10.1186/s12933-025-02689-6. Cardiovasc Diabetol. 2025. PMID: 40128747 Free PMC article.
-
28-day all-cause mortality in patients with alcoholic cirrhosis: a machine learning prediction model based on the MIMIC-IV.Clin Exp Med. 2025 Jun 11;25(1):198. doi: 10.1007/s10238-025-01744-6. Clin Exp Med. 2025. PMID: 40498328 Free PMC article.
-
Predictive performance of stress hyperglycemia ratio for poor prognosis in critically ill patients: a systematic review and dose-response meta-analysis.Eur J Med Res. 2025 Jul 11;30(1):613. doi: 10.1186/s40001-025-02868-x. Eur J Med Res. 2025. PMID: 40646634 Free PMC article. Review.
References
-
- Vaduganathan, M., Mensah, G. A., Turco, J. V., Fuster, V. & Roth, G. A. The Global Burden of Cardiovascular diseases and Risk: a compass for Future Health. J. Am. Coll. Cardiol.80, 2361–2371. 10.1016/j.jacc.2022.11.005 (2022). - PubMed
-
- Duggan, J. P., Peters, A. S., Trachiotis, G. D. & Antevil, J. L. Epidemiology of coronary artery disease. Surg. Clin. North. Am.102, 499–516. 10.1016/j.suc.2022.01.007 (2022). - PubMed
-
- Malakar, A. K. et al. A review on coronary artery disease, its risk factors, and therapeutics. J. Cell. Physiol.234, 16812–16823. 10.1002/jcp.28350 (2019). - PubMed
-
- Vincent, J. L. et al. Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med.2, 380–386. 10.1016/s2213-2600(14)70061-x (2014). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
