

Community versus academic hospital community-acquired pneumonia patients: a nested cohort study
- PMID: 39582027
- PMCID: PMC11587589
- DOI: 10.1186/s41479-024-00143-x
Community versus academic hospital community-acquired pneumonia patients: a nested cohort study
Abstract
Background: Most Canadians receive their care in community hospitals, yet most clinical research is conducted in academic hospitals. This study aims to compare patients with community acquired pneumonia (CAP) treated in academic and community hospitals with respect to their demographics, clinical characteristics, treatments and outcomes.
Methods: This nested observational cohort substudy of the Community Acquired Pneumonia: Toward InnoVAtive Treatment (CAPTIVATE) trial included 1,329 hospitalized adults with CAP recruited between March 1st, 2018 and September 31st, 2023 from 15 Canadian hospitals. Unadjusted and adjusted analyses for age, sex and co-morbidities using logistic, Cox and censored quantile regressions were conducted.
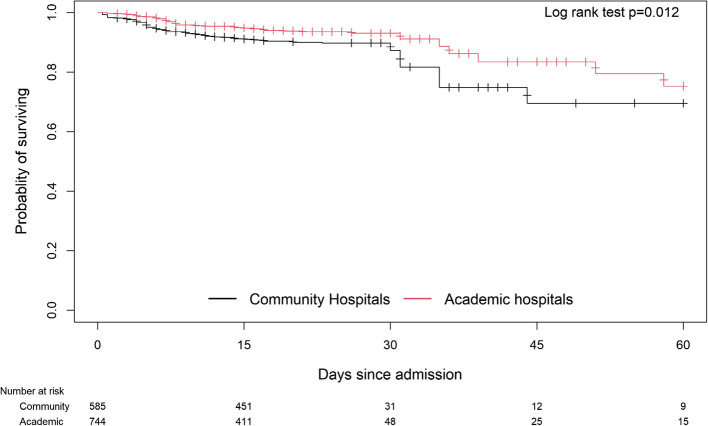
Results: Patients in community hospitals were older (mean [SD] 75.0 [15.7] years vs. 68.3 [16.2] years; p < 0.001), were more likely to be female (49.7% vs. 41.0%, p = 0.002), and had more comorbidities (75.9% vs. 64.8%, p < 0.001). More patients in community hospitals received corticosteroids (49.2% vs. 37.4%, p < 0.001). Community hospital patients had a higher likelihood of developing acute respiratory distress syndrome (OR 3.13, 95% CI: 1.87, 5.24, p = < 0.001), and acute cardiac injury (OR 2.53, 95% CI: 1.33, 4.83, p = 0.005). In unadjusted and adjusted analyses, 28-day mortality difference did not meet statistical significance (OR 1.43, 95% CI: 0.98, 20.7, p = 0.062 and OR 1.23, 95% CI: 0.81, 1.87, p = 0.332, respective).
Conclusion: Patients with CAP in Canadian community and academic hospitals differed with respect to their age, clinical characteristics, treatments and outcomes, emphasizing the importance of including more community hospitals in clinical research studies to ensure the generalizability of results.
Keywords: Community hospital; Community-acquired pneumonia; Corticosteroids; Mortality.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethics approval was received from the University of British Columbia Providence Health Care Research Ethics Board (REB Number: H20-00600) and by each of the participating sites. Consent for publication: Not applicable. Competing interests: Support for CAPTIVATE was obtained from grants to J.A.R. from the Canadian Institutes of Health Research (grant number: 439993) and St. Paul’s Hospital Foundation. J.B. is a recipient of a Providence Health Care Research Scholarship. K.W. is supported by Canadian Institutes of Health Research (CIHR) Foundation Grant (FDN 154311). A.F.T. is the chairholder of the Canada Research Chair in Critical care neurology and trauma. D.C.V. is supported by the Fonds de recherche du Québec – Santé (FRQS) clinician-scientist Senior scholar award. D.C.V. has received funding support from the Jeffrey Modell Foundation, FRQS, and Canadian Institutes of Health Research. D.C.V. has served on advisory boards for: Astra Zeneca; CSL Behring; Novartis Canada; Moderna; Takeda. D.C.V. has received speaker honoraria from: CSL Behring; Merck Canada. DCV has a patent application pending (Electronic Filing System ID: 40101099) unrelated to this work. M.C. reports grants from the Canadian Institutes of Health Research during the conduct of the study and is supported by the Fonds de Recherche du Québec – Santé. M.C. reports personal fees from GEn1E Lifesciences and from nomic bio as a member of the scientific advisory board, as well as honoraria from AstraZeneca, Takeda, Merck, and Pfizer. M.C. reports research support from Cidara therapeutics, from Scynexis, Inc., and from Amplyx Pharmaceutics during the conduct of the study but outside the submitted work. M.C. is the co-founder of Kanvas Biosciences, Inc. and owns equity in the company. M.C. has pending patents, including: i) Methods for detecting tissue damage, graft versus host disease, and infections using cell-free DNA profiling, ii) Methods for assessing the severity and progression of SARS-CoV-2 infections using cell-free DNA pending.
Figures
References
-
- Canadian Institute for Health Information. Hospital beds staffed and in operation 2020–2021. 2022. Available from: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUK....
-
- Carmen. Visible minorities now the majority in 5 B.C. cities. CBCNews; 2017. Available from: https://www.cbc.ca/news/canada/british-columbia/visible-minorities-now-t....
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
