

The Long and Winding Road: Three-year Mortality Following Prescription of Multidrug Antibiotic Treatment for Mycobacterium avium complex Pulmonary Disease in United States Medicare Beneficiaries With Bronchiectasis
- PMID: 39582505
- PMCID: PMC11584409
- DOI: 10.1093/ofid/ofae639
The Long and Winding Road: Three-year Mortality Following Prescription of Multidrug Antibiotic Treatment for Mycobacterium avium complex Pulmonary Disease in United States Medicare Beneficiaries With Bronchiectasis
Abstract
Background/aims: Although increased mortality has been reported among people with Mycobacterium avium complex pulmonary disease (MAC-PD), data are limited on survival associated with various antibiotic regimens used to treat MAC-PD. We conducted a comparative analysis of 3-year mortality in Medicare beneficiaries with bronchiectasis using various MAC-PD regimens.
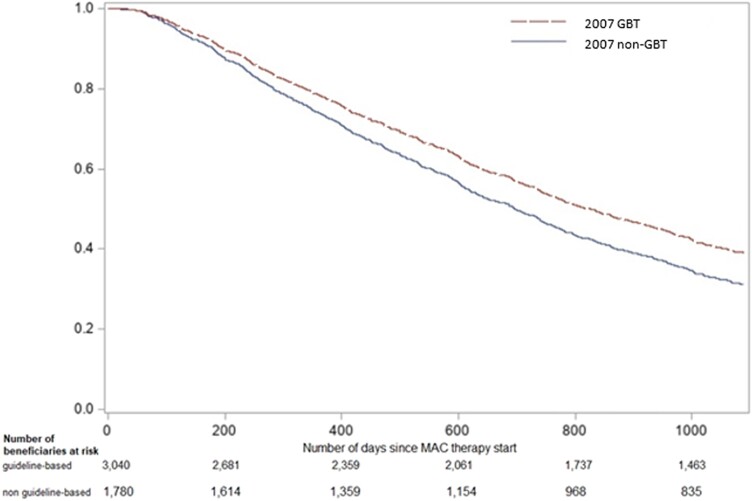
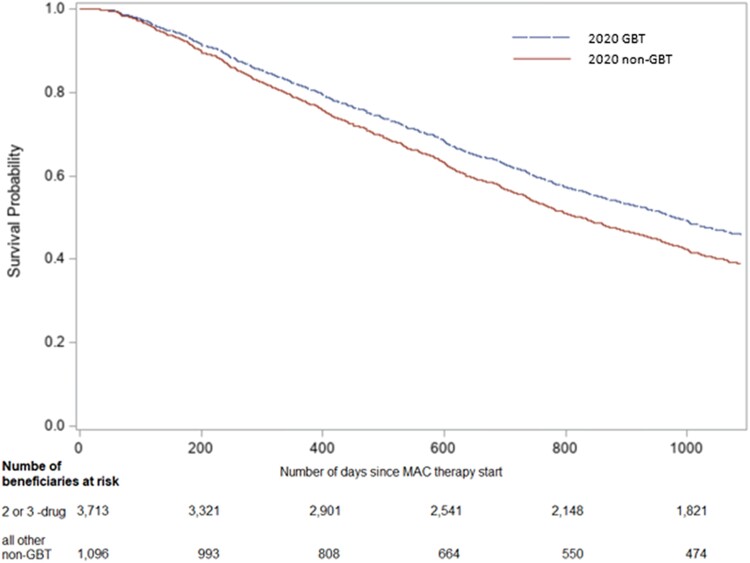
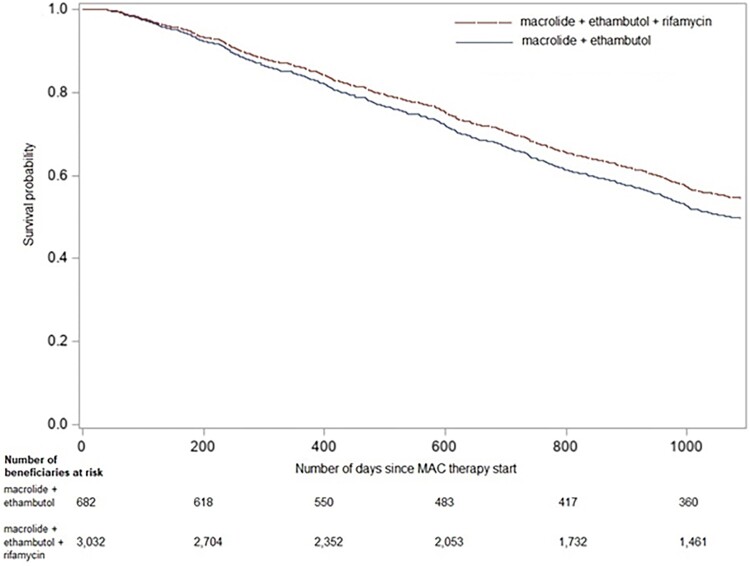
Methods: We included Medicare beneficiaries aged ≥65 years with bronchiectasis (01/2006-12/2014). We limited our cohort to new MAC-PD therapy users. MAC-PD therapy was defined as ≥60-day prescriptions for a macrolide plus ≥1 other MAC-PD antibiotic. Guideline-based therapy (GBT) included a macrolide, ethambutol, and/or rifamycin. Using Cox proportional hazard models, we calculated adjusted hazard ratios (aHR) for death up to 3 years after therapy start between the following groups: (1) 2007 GBT versus non-GBT; (2) 2020 GBT versus non-GBT; and (3) macrolide-ethambutol-rifamycin (3-drug) versus macrolide-ethambutol (2-drug).
Results: We identified 4820 new MAC-PD therapy users, of whom 866 (17.9%) were deceased within 3 years of therapy initiation. Of 3040 (63.1%) beneficiaries prescribed 2007 GBT, 472 (15.5%) were deceased by 3 years, compared to 394 (22.1%) of 1780 (36.9%) prescribed non-GBT (aHR 0.82; 95% confidence interval [CI], .72-.94). We observed a similar trend for 2020 GBT versus non-GBT (aHR 0.81; 95% CI, .70-.94]). Three-year-mortality was similar between those starting 3-drug versus 2-drug regimens (aHR 0.89; 95% CI, .74-1.08]).
Conclusions: Among Medicare new MAC-PD therapy users, 3-year-mortality was higher in those prescribed non-GBT regimens compared to GBT regimens. Whether this finding suggests improved efficacy of GBT and/or differential characteristic of those using non-GBT regimens deserves further study.
Keywords: Mycobacterium avium complex; Nontuberculous mycobacteria; bronchiectasis; evidence based medicine; infectious disease guidelines; mortality; pulmonary infections.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. C.D.V.: Research support from National Institutes of Health, National Heart, Lung, and Blood. Institute grant: K23HL161495. J.H.K.: research support from GSK and Moderna. E.H.: consultant/advisory board AN2, Spero, MannKind. L.S.: none. K.L.W.: Research support from Insmed, Paratek, AN2, Spero, Mannkind. Consultant for Insmed, AN2, Spero, Mannkind.
Figures
References
-
- Winthrop KL, McNelley E, Kendall B, et al. Pulmonary nontuberculous mycobacterial disease prevalence and clinical features: an emerging public health disease. Am J Respir Crit Care Med 2010;182:977–82. - PubMed
-
- Falkinham JO 3rd. Surrounded by mycobacteria: nontuberculous mycobacteria in the human environment. J Appl Microbiol 2009; 107:356–67. - PubMed
-
- Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 2007; 175:367–416. - PubMed
-
- Boyle DP, Zembower TR, Qi C. Relapse versus reinfection of Mycobacterium avium complex pulmonary disease. Patient characteristics and macrolide susceptibility. Ann Am Thorac Soc 2016; 13:1956–61. - PubMed
LinkOut - more resources
Full Text Sources
