

Pre-emptive use of glucose 5% as the standard drug solvent reduces hypernatremia in critically ill patients
- PMID: 39582778
- PMCID: PMC11584513
- DOI: 10.1093/ckj/sfae328
Pre-emptive use of glucose 5% as the standard drug solvent reduces hypernatremia in critically ill patients
Abstract
Background: Hypernatremia presents a common complication in intensive care unit (ICU) patients, associated with increased mortality and length of stay. This study investigates the effect of sodium chloride 0.9% compared with glucose 5% solution as the standard intravenous drug diluent on the prevalence of hypernatremia in a medical ICU.
Methods: This is a retrospective before-and-after study comparing two consecutive patient groups before and after the standard drug solvent was changed from sodium chloride 0.9% to glucose 5% solution for compatible medications. A total of 265 adult COVID-19 patients admitted between October 2020 and March 2021 to the study ICU were included, with 161 patients in the timeframe when sodium chloride 0.9% was employed as the standard drug solvent and 104 patients when glucose 5% was used. Routine sodium measurements from arterial and venous blood gases, along with heparinized lithium plasma, were analyzed. The daily sodium concentrations and the prevalence of severe hypernatremia (>150 mmol/l) were assessed during the first 8 days after ICU admission.
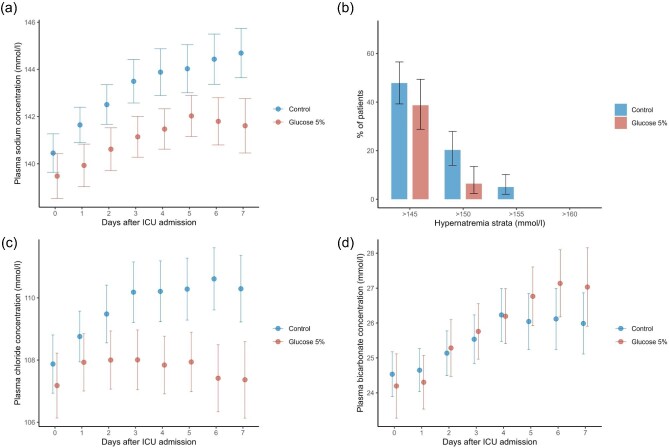
Results: Baseline characteristics were similar between the two groups. The cumulative volume of intravenous drug diluents was comparable. In the glucose 5% group, about half of the total drug diluent volume was glucose 5% [mean (SD): 2251.6 (2355.4) ml], compared to 135.0 (746.9) ml (P < .001) in the control group. Average sodium concentrations diverged after day two, with the glucose 5% group consistently showing lower sodium levels (mean difference of ∼2.5 mmol/l). Severe hypernatremia occurred less frequently in the glucose 5% group (6.6% vs. 20%).
Conclusion: Glucose 5% solution as the standard intravenous drug solvent significantly reduced sodium concentrations and the occurrence of severe hypernatremia. This simple modification in solvent choice may serve as a preventive strategy against hypernatremia in the ICU. Further prospective research is necessary to determine associated clinical outcomes.
Trial registration: The trial was registered in the German Clinical Trials Register (DRKS00031877).
Keywords: drug diluent; drug solvent; glucose 5%; hypernatremia; sodium chloride 0.9%.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
None declared.
Figures



References
LinkOut - more resources
Full Text Sources
