

Treatment-related survival patterns in diffuse intrinsic pontine glioma using a historical cohort: A report from the European Society for Pediatric Oncology DIPG/DMG Registry
- PMID: 39582811
- PMCID: PMC11582646
- DOI: 10.1093/noajnl/vdae155
Treatment-related survival patterns in diffuse intrinsic pontine glioma using a historical cohort: A report from the European Society for Pediatric Oncology DIPG/DMG Registry
Abstract
Background: Our aim is to investigate the association of treatment with survival in patients with diffuse intrinsic pontine glioma (DIPG) by examining 6 historical treatment paths.
Methods: We retrospectively analyzed data from 409 patients with radiologically centrally reviewed DIPG, sourced from the German Society of Pediatric Oncology and Hematology HIT-HGG trial database and the SIOPE-DIPG/DMG Registry. Survival outcomes were estimated using the Kaplan-Meier method, and univariable and multivariable Cox proportional hazard models were estimated to study treatment effects.
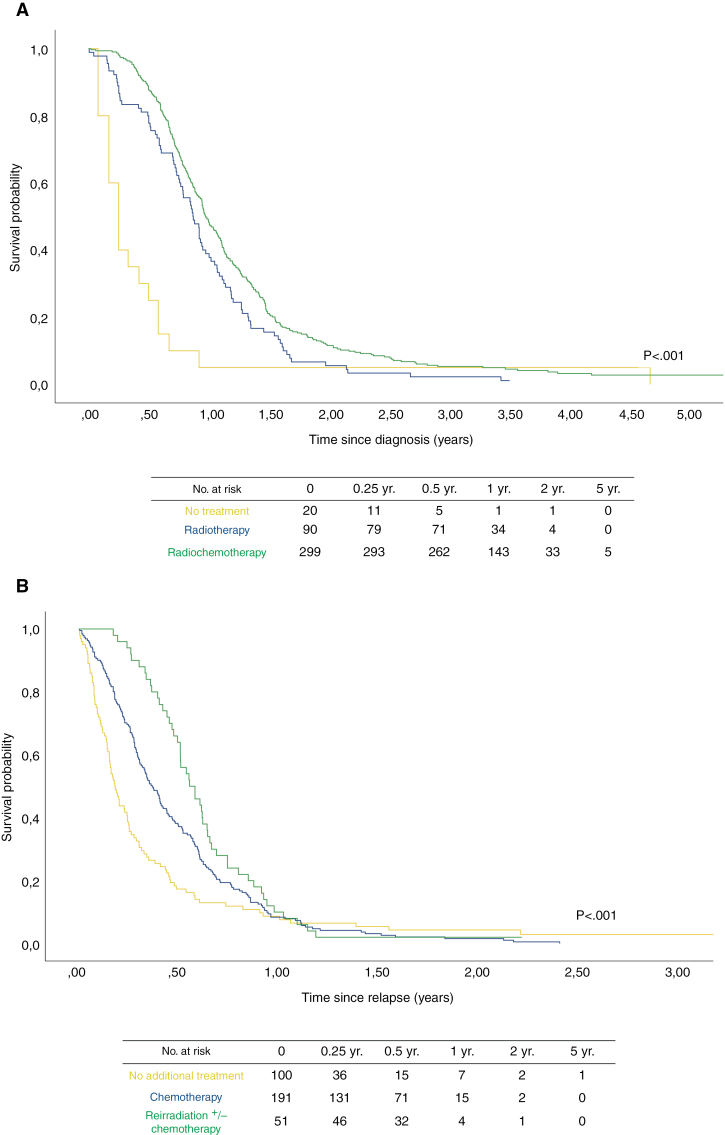
Results: The median overall survival (OS) from diagnosis was 11.2 months (95% confidence interval [CI], 10.5-11.9). Patients who by choice received no frontline treatment had an OS of 3.0 months (95% CI, 2.0-4.0), while those treated with radiation therapy (RT) alone had a median OS of 10.4 months (95% CI, 9.1-11.8). Those receiving RT combined with chemotherapy had the longest median OS of 11.7 months (95% CI, 10.8-12.6). The median post-progression survival (PPS) was 4.1 months (95% CI, 3.5-4.7). Patients who relapsed and did not receive treatment had a PPS of 2.2 months (95% CI, 1.8-2.6), while those treated with chemotherapy alone had a PPS of 4.4 months (95% CI, 3.7-5.0), and those who underwent reirradiation, with or without chemotherapy, had the longest survival after relapse of 6.6 months (95% CI, 5.3-8.0). Treatment differences remained significant in multivariable analysis adjusted for age and symptom duration in both diagnosis and relapse setting.
Conclusions: This study shows increased survival outcomes associated with radiation and chemotherapy treatment or a combination thereof, at diagnosis and relapse, in a historical DIPG cohort.
Keywords: DIPG; diffuse intrinsic pontine glioma; diffuse midline glioma; historical control; registry.
© The Author(s) 2024. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Conflict of interest statement
None declared.
Figures
References
-
- Langmoen IA, Lundar T, Storm-Mathisen I, Lie SO, Hovind KH.. Management of pediatric pontine gliomas. Childs Nerv Syst. 1991;7(1):13–15. - PubMed
-
- Hoffman LM, Veldhuijzen van Zanten SEM, Colditz N, et al. Clinical, radiologic, pathologic, and molecular characteristics of long-term survivors of diffuse intrinsic pontine glioma (DIPG): a collaborative report from the International and European Society for Pediatric Oncology DIPG Registries. J Clin Oncol. 2018;36(19):1963–1972. - PMC - PubMed
-
- van Walraven C, Davis D, Forster AJ, Wells GA.. Time-dependent bias was common in survival analyses published in leading clinical journals. J Clin Epidemiol. 2004;57(7):672–682. - PubMed
LinkOut - more resources
Full Text Sources