

Clinical and Radiological Outcomes of Anchored Stand-Alone Cage Compared to Conventional Plating in Multilevel Anterior Cervical Discectomy and Fusion: A Systematic Review
- PMID: 39583521
- PMCID: PMC11586081
- DOI: 10.7759/cureus.72386
Clinical and Radiological Outcomes of Anchored Stand-Alone Cage Compared to Conventional Plating in Multilevel Anterior Cervical Discectomy and Fusion: A Systematic Review
Abstract
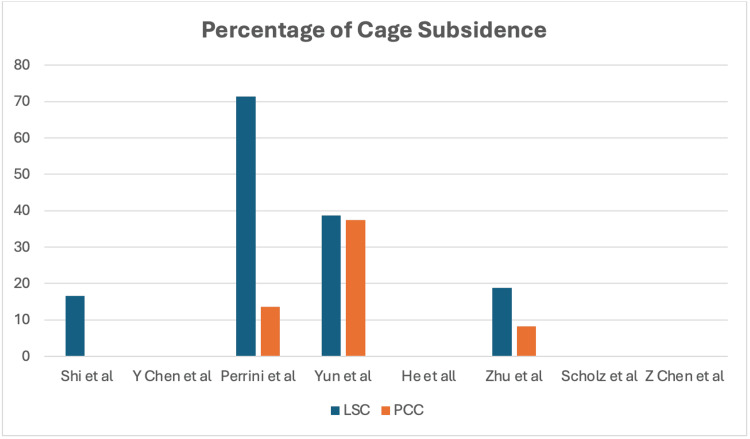
Multilevel cervical degenerative disc disease (cDDD) is typically treated through anterior cervical discectomy and fusion (ACDF). Traditionally, the plate-cage construct (PCC) has been utilized, though alternatives such as the locking stand-alone cage (LSC) have become popular. This systematic review aims to assess differences in clinical and radiological outcomes between LSC and PCC methods in the ACDF management of multilevel cDDD by aggregating existing literature. A comprehensive search of five electronic databases (PubMed, Medline, Ovid, Embase, and Cochrane) was conducted from 2015 to 2022 following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The comparative studies were assessed using the Methodological Index for Non-randomized Studies (MINORS) criteria and the two randomized controlled trials (RCTs) were assessed using the Jadad scale for RCT. Eight studies met the inclusion criteria, comprising a total cohort of 516 contiguous multilevel cDDD cases treated via ACDF, with 254 (49%) managed with PCC and 262 (51%) treated with LSC. The comparative outcomes assessed included the rate of subsidence and the rate of postoperative dysphagia. The LSC approach exhibited a higher incidence of cage subsidence compared to PCC. Conversely, dysphagia was observed more frequently in patients receiving PCC compared to those treated with LSC. Clinical outcomes and functional scores did not reveal significant differences. Clinical measures such as the Japanese Orthopaedic Association (JOA) score, Neck Disability Index (NDI), visual analog scale (VAS), and Odom's and Robinson's criteria revealed no significant differences between treatment groups in seven of the studies. However, one of the included studies reported a statistically significant improvement in the LSC group for VAS and Odom's criteria. The incidence of cage subsidence in ACDF surgery varies depending on the cage type employed. Among the reviewed studies, the LSC group exhibited a higher incidence of subsidence compared to the PCC group, with the exception of one study that reported no cases of subsidence. Variability in subsidence rates across studies may be attributed to differences in surgical techniques, patient demographics, and follow-up periods. Further research is necessary to investigate associated risk factors and to develop strategies aimed at minimizing this complication in ACDF procedures.
Keywords: anchored; anterior; anterior plate construct; arthrodesis; cervical discectomy; fusion; plate; stand-alone.
Copyright © 2024, Ghobrial et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures


Similar articles
-
Clinical outcomes of locking stand-alone cage versus anterior plate construct in two-level anterior cervical discectomy and fusion: a systematic review and meta-analysis.Eur Spine J. 2019 Jan;28(1):199-208. doi: 10.1007/s00586-018-5811-x. Epub 2018 Nov 2. Eur Spine J. 2019. PMID: 30390163
-
A comparison of anterior cervical discectomy and fusion (ACDF) using self-locking stand-alone polyetheretherketone (PEEK) cage with ACDF using cage and plate in the treatment of three-level cervical degenerative spondylopathy: a retrospective study with 2-year follow-up.Eur Spine J. 2016 Jul;25(7):2255-62. doi: 10.1007/s00586-016-4391-x. Epub 2016 Feb 23. Eur Spine J. 2016. PMID: 26906171
-
Comparison of Stand-Alone Anchored Spacer and Plate-Cage Construct for Surgical Treatment of Multilevel Cervical Degenerative Spondylopathy: A Meta-Analysis.Global Spine J. 2025 Sep;15(7):3364-3378. doi: 10.1177/21925682251327599. Epub 2025 Mar 25. Global Spine J. 2025. PMID: 40129298 Free PMC article. Review.
-
Comparison of the effectiveness of zero-profile device and plate cage construct in the treatment of one-level cervical disc degenerative disease combined with moderate to severe paraspinal muscle degeneration.Front Endocrinol (Lausanne). 2023 Dec 6;14:1283795. doi: 10.3389/fendo.2023.1283795. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38125794 Free PMC article.
-
Locking stand-alone cage versus anterior plate construct in anterior cervical discectomy and fusion: a systematic review and meta-analysis based on randomized controlled trials.Eur Spine J. 2020 Nov;29(11):2734-2744. doi: 10.1007/s00586-020-06561-x. Epub 2020 Aug 8. Eur Spine J. 2020. PMID: 32770359
References
-
- Systematic review of cohort studies comparing surgical treatments for cervical spondylotic myelopathy. Cunningham MR, Hershman S, Bendo J. Spine (Phila Pa 1976) 2010;35:537–543. - PubMed
-
- Anterior approaches to fusion of the cervical spine: a metaanalysis of fusion rates. Fraser JF, Härtl R. J Neurosurg Spine. 2007;6:298–303. - PubMed
-
- The efficacy of plate construct augmentation versus cage alone in anterior cervical fusion. Song KJ, Taghavi CE, Lee KB, Song JH, Eun JP. Spine (Phila Pa 1976) 2009;34:2886–2892. - PubMed
-
- Anterior cervical discectomy and fusion associated complications. Fountas KN, Kapsalaki EZ, Nikolakakos LG, et al. Spine (Phila Pa 1976) 2007;32:2310–2317. - PubMed
-
- The incidence of adjacent segment disease requiring surgery after anterior cervical diskectomy and fusion: estimation using an 11-year comprehensive nationwide database in Taiwan. Wu JC, Liu L, Wen-Cheng H, et al. Neurosurgery. 2012;70:594–601. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous