

Response-Adaptive Surgical Timing in Neoadjuvant Immunotherapy Demonstrates Enhanced Pathologic Treatment Response in Head and Neck Squamous Cell Carcinoma
- PMID: 39585339
- PMCID: PMC11973698
- DOI: 10.1158/1078-0432.CCR-24-0037
Response-Adaptive Surgical Timing in Neoadjuvant Immunotherapy Demonstrates Enhanced Pathologic Treatment Response in Head and Neck Squamous Cell Carcinoma
Abstract
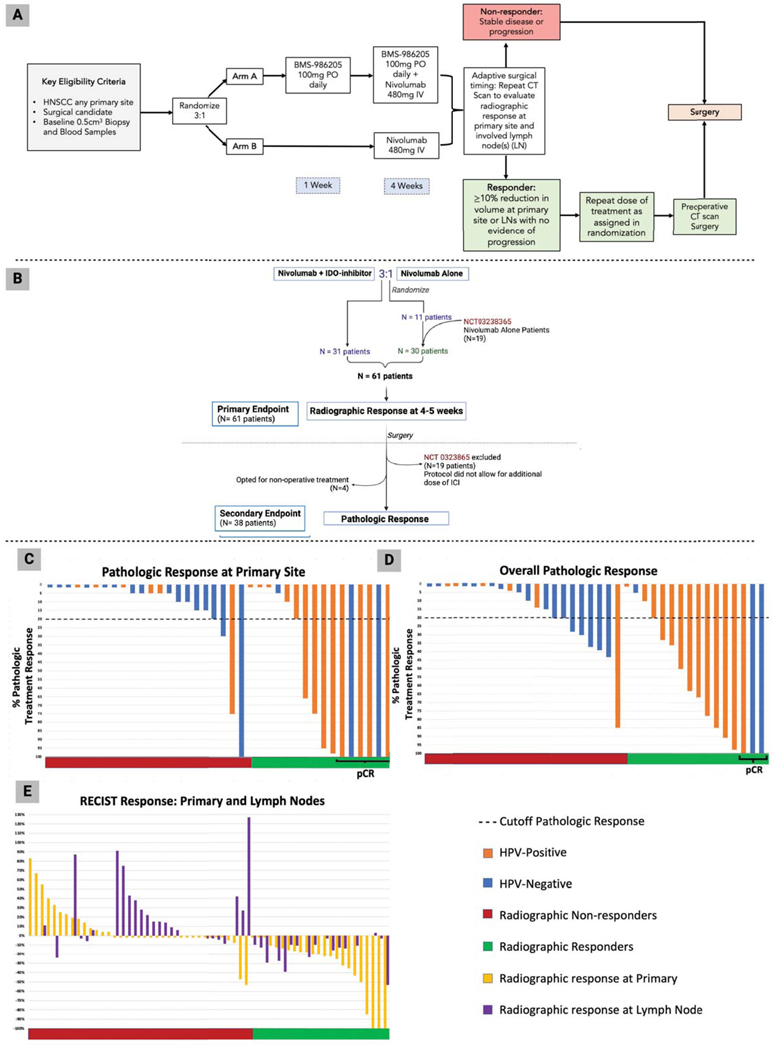
Purpose: We evaluated whether indoleamine 2,3-dioxygenase (IDO1) inhibitor (IDOi) BMS986205 + PD-1 inhibitor nivolumab enhanced T-cell activity and augmented immune-mediated antitumor responses in untreated, resectable head and neck squamous cell carcinoma (HNSCC). We employed response-adaptive surgical timing to identify responders to immunotherapy and enhance their response.
Patients and methods: Patients with HNSCC were 3:1 randomized to receive nivolumab with or without BMS986205 orally daily (NCT03854032). In the combination arm, BMS986205 was initiated 7 days prior to nivolumab. Patients were stratified by human papillomavirus (HPV) status. Response-adaptive surgical timing involved response assessment by radiographic criteria 4 weeks after treatment with nivolumab in both arms. Nonresponders underwent surgical resection, whereas responders received 4 more weeks of randomized therapy before surgery. Biomarker analysis utilized pathologic treatment response (pTR) and RNA sequencing.
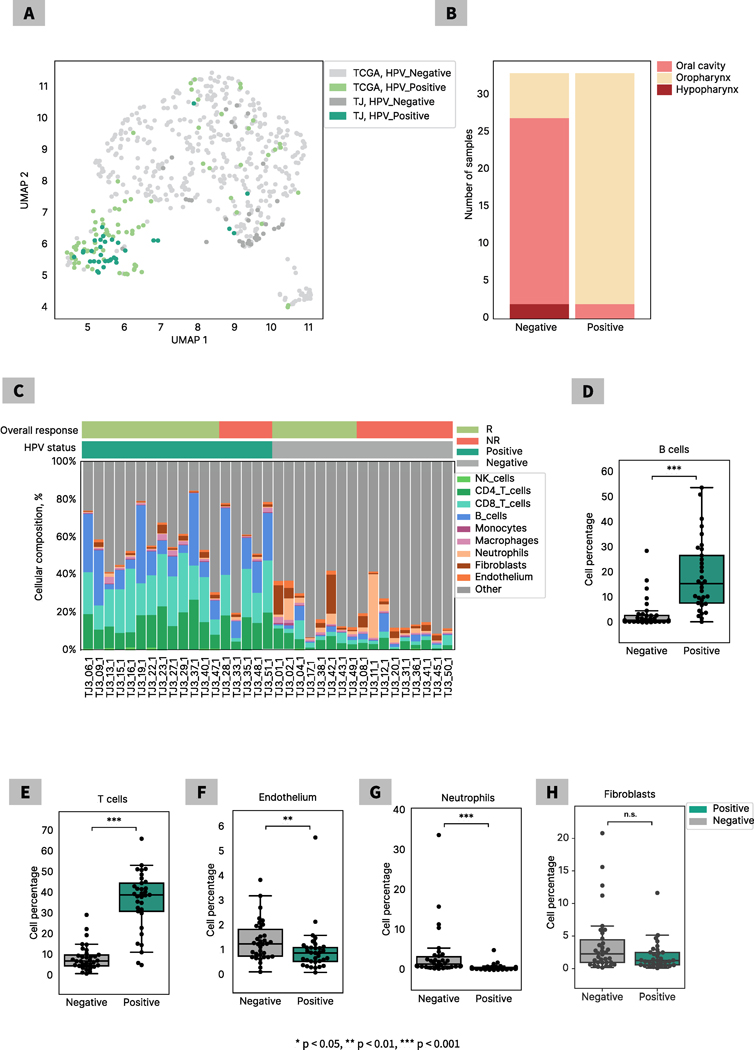
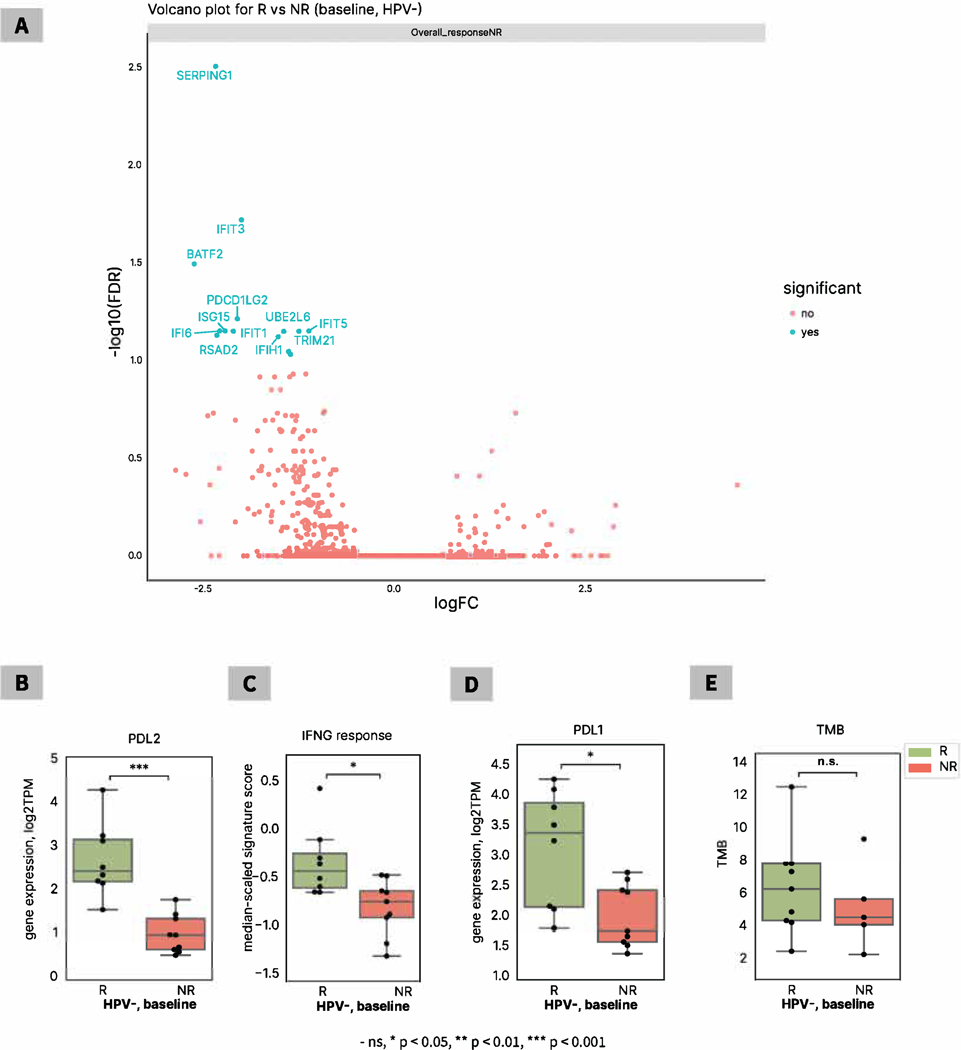
Results: Forty-two patients were enrolled, and the addition of IDOi to nivolumab did not result in greater rate of radiographic response (P = 0.909). Treatment was well tolerated, with only 2 (5%) patients experiencing grade 3 immune-related adverse events. The addition of IDOi augmented rates of pTR in patients with high baseline IDO1 RNA expression (P < 0.05). Response-adaptive surgical timing demonstrated reliability in differentiating pathologic responders versus nonresponders (P = 0.009). A pretreatment NK cell signature, PD-L1 status, and IFN-γ expression in the HPV- cohort correlated with response. The HPV+ cohort found B-cell and cancer-associated fibroblast signatures predictive of response/nonresponse.
Conclusions: Response-adaptive surgical timing enhanced treatment response. IDOi BMS986205 augmented pTR in patients with high IDO1 expression in baseline samples, indicating a need for identifying and targeting resistant nodes to immunotherapy. HPV status-dependent signatures predicting response to immunotherapy in HNSCC warrant further study.
©2024 American Association for Cancer Research.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
