

Survival outcomes fifteen years after minimally invasive esophagectomy
- PMID: 39585588
- PMCID: PMC11589040
- DOI: 10.1007/s12672-024-01567-z
Survival outcomes fifteen years after minimally invasive esophagectomy
Abstract
Background and objectives: Minimally invasive esophagectomy (MIO) offers a less traumatic resection for cancer patients resulting in improved quality of life. Concerns about the oncological efficacy of the procedure and potential impact on survival may have limited its wider adoption. This study reports survival outcomes fifteen years after patients underwent a total MIO for esophageal cancer.
Methods: A single-centre analysis of survival outcomes was conducted on all patients who underwent MIO between 2004 and 2010 and had completed at least 15-years follow-up. Actual overall survival (OS) and disease-free survival (DFS) were evaluated with the Kaplan-Meier method. The pattern of association of patient factors with survival was assessed with the Cox regression analysis.
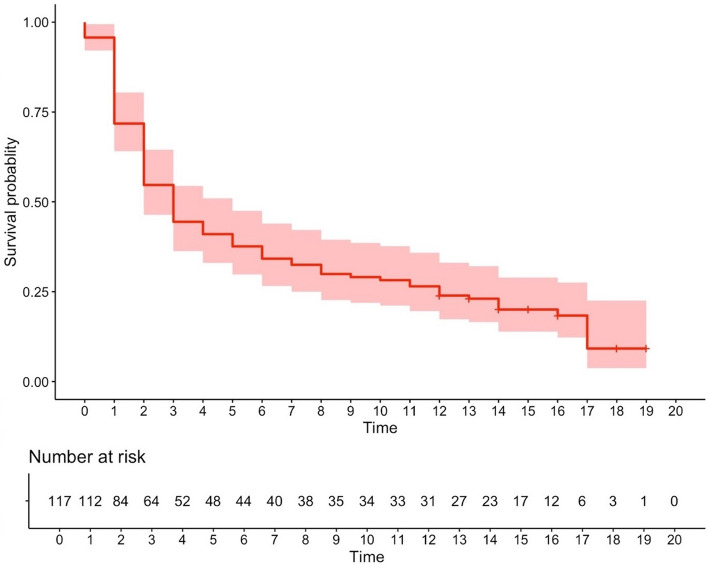
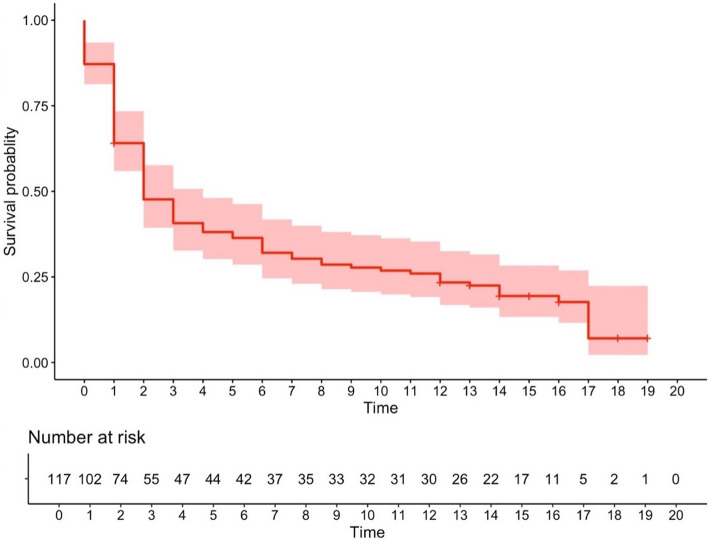
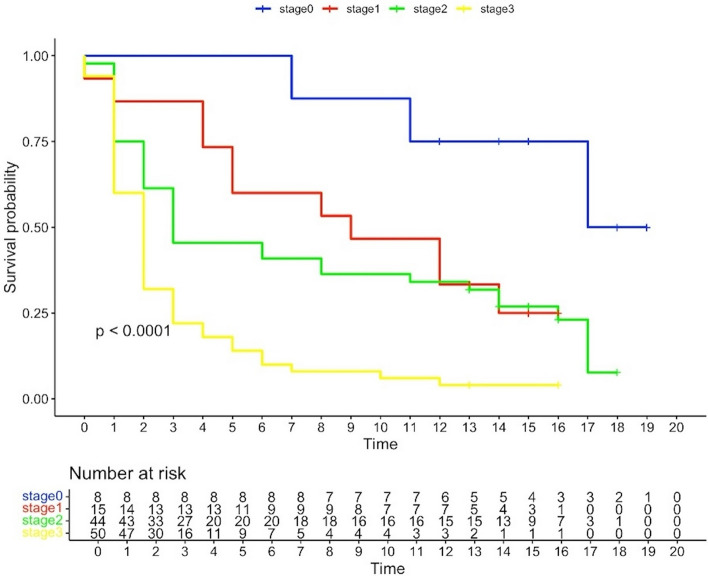
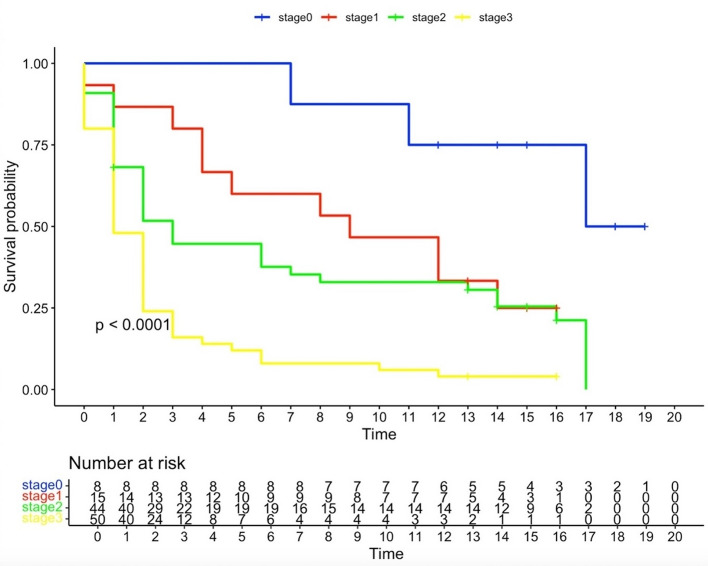
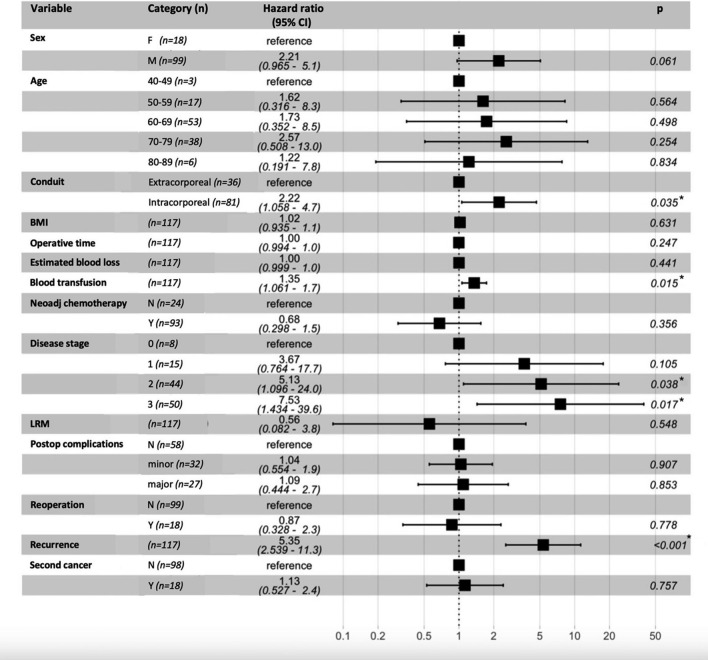
Results: A total of 121 patients underwent resection, with 4 (3.3%) in-patient deaths. With a median follow-up time of 15.2 years, the median OS was 41 months. At 15-years there were 20 survivors (17.1%), with numbers at 10 and 5 years being 34 (29.1%) and 45 (38.5%) respectively. Median DFS was 27 months, with 19 (16.2%) patient disease free at 15 years, and 32 (27.4%) and 38 (32.5%) at 10 and 5 years respectively. Predictors of poor survival were the intracorporeal fashioning of the gastric conduit, perioperative blood transfusions, advanced disease stage and recurrence.
Conclusions: Long term survival outcomes following MIO support its increasing recognition as the standard of care as for curative resection in esophageal cancer.
Keywords: Esophageal cancer; Minimally invasive esophagectomy; Survival.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study had been registered and approved by the Royal Devon and Exeter NHS Foundation Trust Governance Board—reference number 24–1389. The Governance Board acted as an advisory panel not as an ethics committee. The study protocol was submitted to the Governance Board; given that the research was limited to secondary use of information previously collected in the course of normal care, and data were fully anonymised, the study did not fill the criteria to require review by the research ethics committee nor patients' consent form, as per the NHS Health Research Authority guidelines ( https://www.hra-decisiontools.org.uk/ethics/docs/Algorithm%20-%20Does%20my%20project%20require%20REC%20review%20v2.0%2020200304.pdf ). Hence, participants’ consent to the study was not obtained. Data transparency: The dataset analysed during the current study is not publicly available, in accordance to the Confidentiality Policy in force at the Royal Devon University Healthcare NHS Foundation Trust; this is a legal requirement under the Data Protection Act 2018 (United Kingdom). Data are available from the corresponding author on reasonable request. Competing interests: The authors declare no competing interests.
Figures
References
-
- Low DE, Kuppusamy MK, Alderson D, Cecconello I, Chang AC, Darling G, Davies A, D’Journo XB, Gisbertz SS, Griffin SM, Hardwick R, Hoelscher A, Hofstetter W, Jobe B, Kitagawa Y, Law S, Mariette C, Maynard N, Morse CR, Nafteux P, Pera M, Pramesh CS, Puig S, Reynolds JV, Schroeder W, Smithers M, Wijnhoven BPL. Benchmarking complications associated with esophagectomy. Ann Surg. 2019;269(2):291–8. 10.1097/SLA.0000000000002611. (PMID: 29206677). - DOI - PubMed
-
- Nuytens F, Dabakuyo-Yonli TS, Meunier B, Gagnière J, Collet D, D’Journo XB, Brigand C, Perniceni T, Carrère N, Mabrut JY, Msika S, Peschaud F, Prudhomme M, Markar SR, Piessen G. Fédération de Recherche en Chirurgie (FRENCH) and French Eso-Gastric tumors (FREGAT) working groups. Five-year survival outcomes of hybrid minimally invasive esophagectomy in esophageal cancer: results of the Miro randomized clinical trial. JAMA Surg. 2021;156(4):323–32. 10.1001/jamasurg.2020.7081. - DOI - PMC - PubMed
-
- Gottlieb-Vedi E, Kauppila JH, Malietzis G, Nilsson M, Markar SR, Lagergren J. Long-term survival in esophageal cancer after minimally invasive compared to open esophagectomy: a systematic review and meta-analysis. Ann Surg. 2019;270(6):1005–17. 10.1097/SLA.0000000000003252. (PMID: 30817355). - DOI - PubMed
LinkOut - more resources
Full Text Sources