

Lipid storage myopathy associated with sertraline treatment is an acquired mitochondrial disorder with respiratory chain deficiency
- PMID: 39586906
- PMCID: PMC11588938
- DOI: 10.1007/s00401-024-02830-x
Lipid storage myopathy associated with sertraline treatment is an acquired mitochondrial disorder with respiratory chain deficiency
Abstract
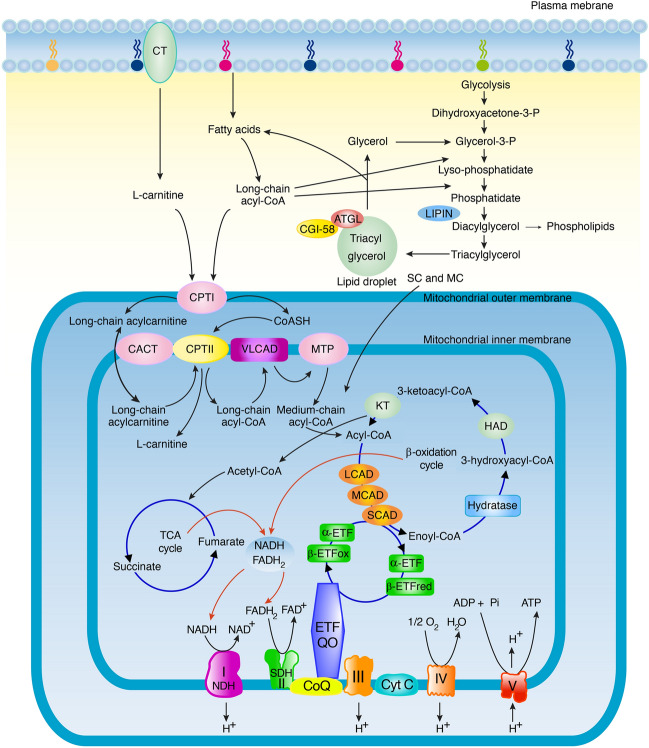
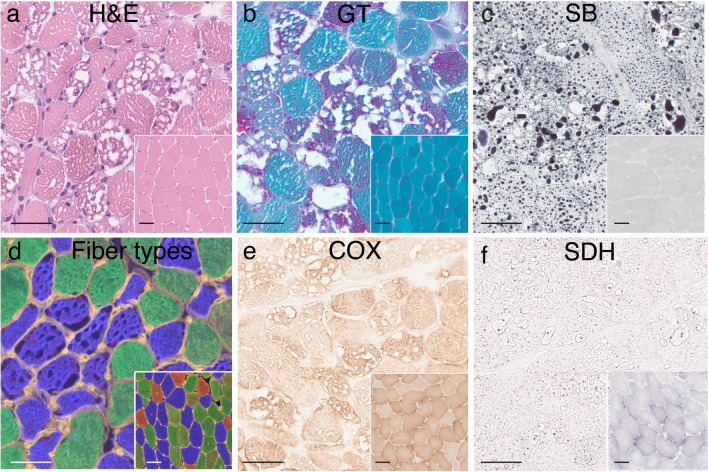
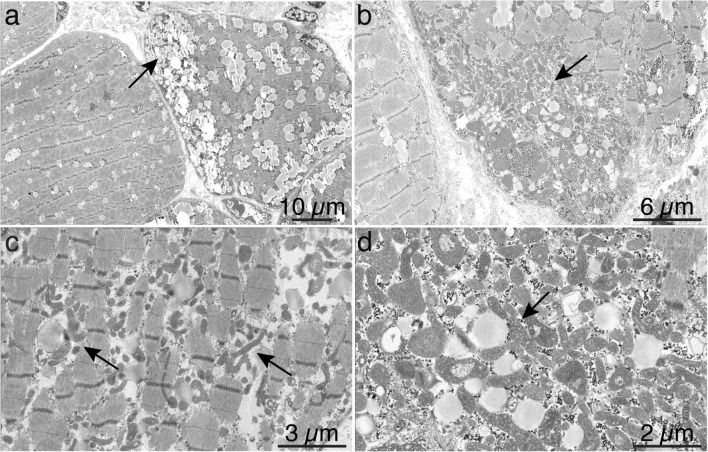
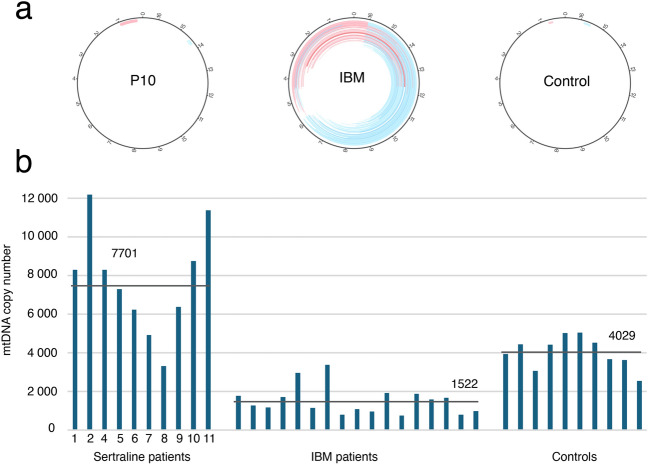
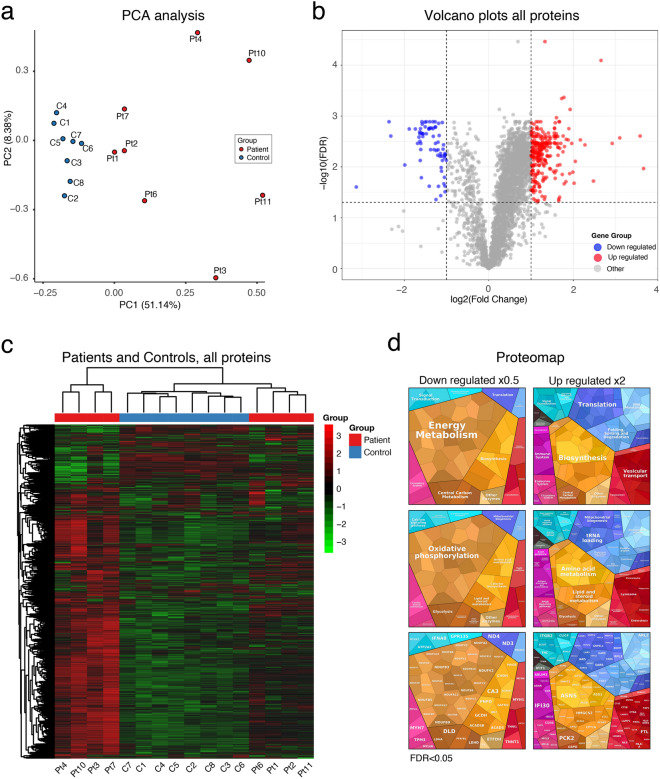
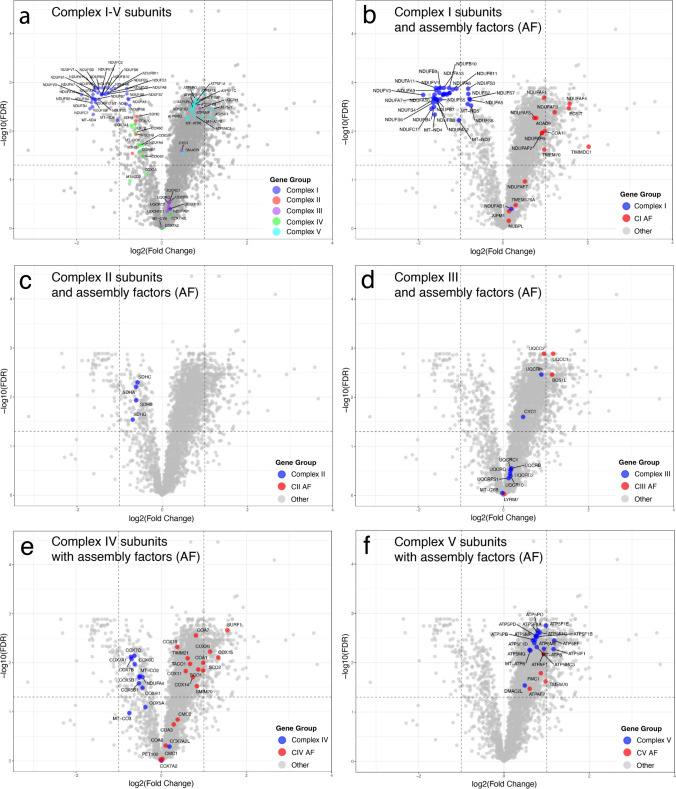
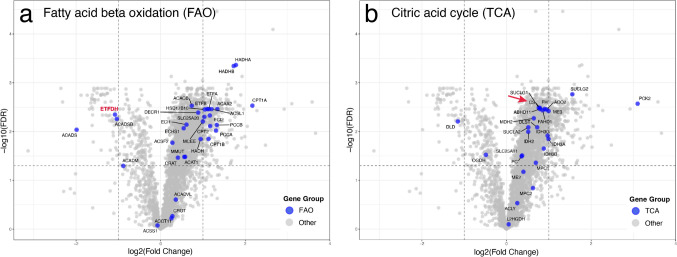
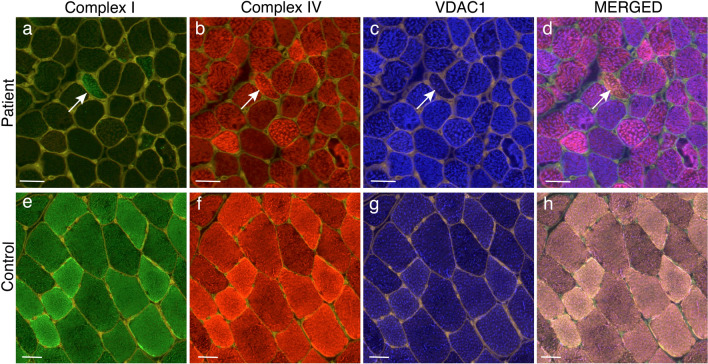
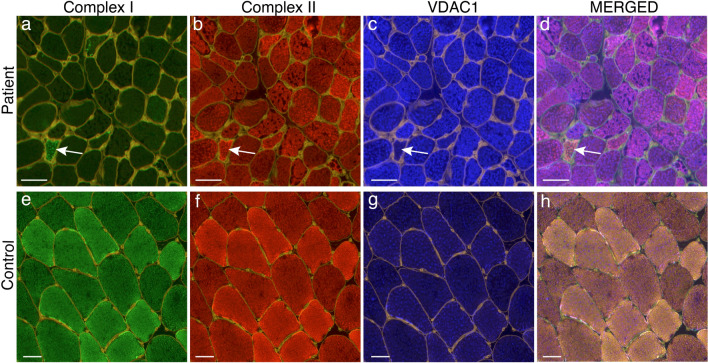
Lipid storage myopathies are considered inborn errors of metabolism affecting the fatty acid metabolism and leading to accumulation of lipid droplets in the cytoplasm of muscle fibers. Specific diagnosis is based on investigation of organic aids in urine, acylcarnitines in blood and genetic testing. An acquired lipid storage myopathy in patients treated with the antidepressant drug sertraline, a serotonin reuptake inhibitor, has recently emerged as a new tentative differential diagnosis. We analyzed the muscle biopsy tissue in a group of 11 adult patients with muscle weakness and lipid storage myopathy which developed at a time when they were on sertraline treatment. This group comprise most patients with lipid storage myopathies in western Sweden during the recent nine-year period. By enzyme histochemistry, electron microscopy, quantitative proteomics, immunofluorescence of the respiratory chain subunits, western blot and genetic analyses we demonstrate that muscle tissue in this group of patients exhibit a characteristic morphological and proteomic profile. The patients also showed an acylcarnitine profile in blood suggestive of multiple acyl-coenzyme A dehydrogenase deficiency, but no genetic explanation was found by whole genome or exome sequencing. By proteomic analysis the muscle tissue revealed a profound loss of Complex I subunits from the respiratory chain and to some extent also deficiency of Complex II and IV. Most other components of the respiratory chain as well as the fatty acid oxidation and citric acid cycle were upregulated in accordance with the massive mitochondrial proliferation. The respiratory chain deficiency was verified by immunofluorescence analysis, western blot analysis and enzyme histochemistry. The typical ultrastructural changes of the mitochondria included pleomorphism, dark matrix and frequent round osmiophilic inclusions. Our results show that lipid storage myopathy associated with sertraline treatment is a mitochondrial disorder with respiratory chain deficiency and is an important differential diagnosis with characteristic features.
Keywords: Lipid storage myopathy; Metabolic crisis; Multiple acyl-CoA dehydrogenase deficiency; Muscle weakness; SSRI; Sertraline.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interests: The authors declare no competing interests. Ethical approval: This study was conducted according to the Declaration of Helsinki and approved by the Swedish Ethical Review Authority, approval number 2023-07591-01. All included patients gave their written informed consent to participate.
Figures
References
-
- Benarroch L, Bonne G, Rivier F, Hamroun D (2024) The 2024 version of the gene table of neuromuscular disorders (nuclear genome). Neuromuscul Disord 34:126–170. 10.1016/j.nmd.2023.12.007 - PubMed
-
- Bousman CA, Stevenson JM, Ramsey LB, Sangkuhl K, Hicks JK, Strawn JR et al (2023) Clinical pharmacogenetics implementation consortium (CPIC) guideline for CYP2D6, CYP2C19, CYP2B6, SLC6A4, and HTR2A genotypes and serotonin reuptake inhibitor antidepressants. Clin Pharmacol Ther 114:51–68. 10.1002/cpt.2903 - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
- ALFGBG-965898/The Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement
- ALFGBG-716821/The Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement
- GLS-999464/The Gothenburg Society of Medicine
- 2018-02821/The Swedish Research Council
LinkOut - more resources
Full Text Sources
Medical
