

APOE4 and age affect the brain entorhinal cortex structure and blood arachidonic acid and docosahexaenoic acid levels after mild TBI
- PMID: 39587176
- PMCID: PMC11589616
- DOI: 10.1038/s41598-024-80153-3
APOE4 and age affect the brain entorhinal cortex structure and blood arachidonic acid and docosahexaenoic acid levels after mild TBI
Abstract
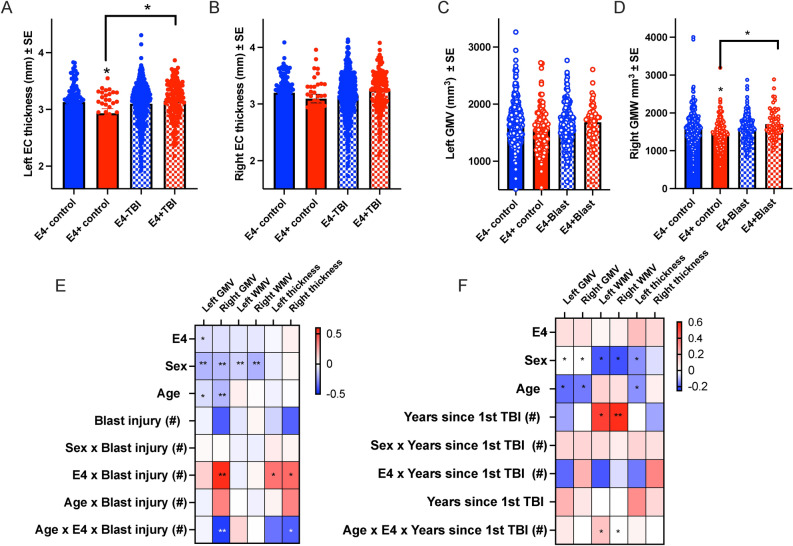
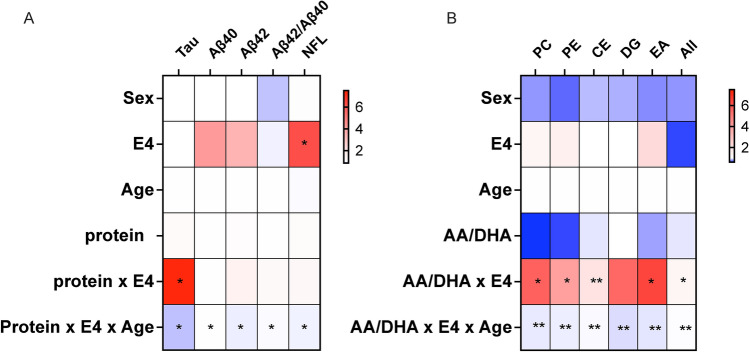
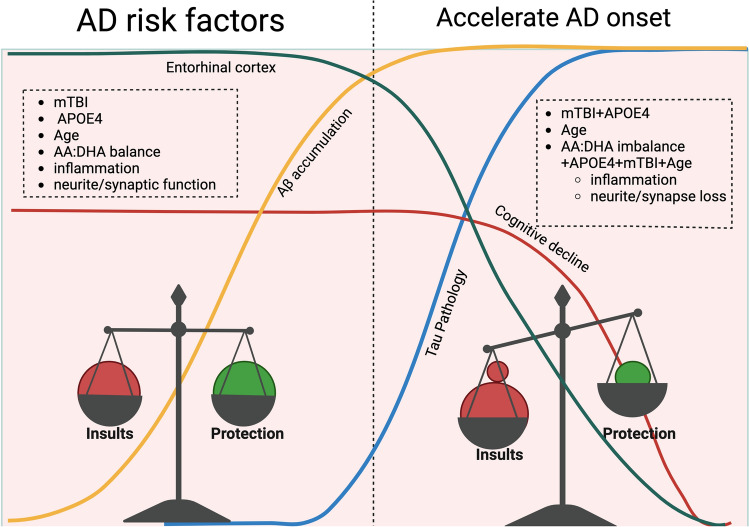
A reduction in the thickness and volume of the brain entorhinal cortex (EC), together with changes in blood arachidonic acid (AA) and docosahexaenoic acid (DHA), are associated with Alzheimer's disease (AD) among apolipoprotein E ε4 carriers. Magnetic Resonance Imaging (n = 631) and plasma lipidomics (n = 181) were performed using the LIMBIC/CENC cohort to examine the influence of ε4 on AA- and DHA-lipids and EC thickness and volume in relation to mild traumatic brain injury (mTBI). Results showed that left EC thickness was higher among ε4 carriers with mTBI. Repeated mTBI (r-mTBI) was associated with reduced right EC thickness after controlling for ε4, age and sex. Age, plus mTBI chronicity were linked to increased EC White Matter Volume (WMV). After controlling for age and sex, the advancing age of ε4 carriers with blast mTBI was associated with reduced right EC Grey Matter Volume (GMV) and thickness. Among ε4 carriers, plasma tau and Aβ40 were associated with mTBI and blast mTBI, respectively. Chronic mTBI, ε4 and AA to DHA ratios in phosphatidylcholine, ethanolamides, and phosphatidylethanolamine were associated with decreased left EC GMV and WMV. Further research is needed to explore these as biomarkers for detecting AD pathology following mTBI.
Keywords: Apolipoprotein E; Arachidonic acid; Blast injury; Docosahexaenoic acid; Entorhinal cortex; Repetitive mild traumatic brain injury; Traumatic brain injury.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval: The views, opinions, interpretations, conclusions and recommendations expressed in this manuscript are those of the authors and do not reflect the official policy of the Department of the Navy, Department of the Army, Department of Defense, Department of Veterans Affairs or the U.S. Government.
Figures


References
MeSH terms
Substances
Grants and funding
- I01 RX002172/RX/RRD VA/United States
- I01 RX002174/RX/RRD VA/United States
- I01 CX002097, I01 CX002096, I01 HX003155, I01 RX003444, I01 RX003443, I01 RX003442, I01 CX001135, I01 CX001246, I01 RX001774, I01 RX 001135, I01 RX 002076, I01 RX 001880, I01 RX 002172, I01 RX 002173, I01 RX 002171, I01 RX 002174, and I01 RX 002170, I01 CX001820/U.S. Department of Veterans Affairs
- I01 CX001135/CX/CSRD VA/United States
- UL1 TR002538/TR/NCATS NIH HHS/United States
- I01 RX003443/RX/RRD VA/United States
- I01 RX001880/RX/RRD VA/United States
- I01 RX002171/RX/RRD VA/United States
- I01 HX003155/HX/HSRD VA/United States
- I01 RX002076/RX/RRD VA/United States
- I01 CX001246/CX/CSRD VA/United States
- I01 RX002170/RX/RRD VA/United States
- UL1 TR000105/TR/NCATS NIH HHS/United States
- I01 RX002173/RX/RRD VA/United States
- AZ160065/Congressionally Directed Medical Research Programs
- UL1 TR001067/TR/NCATS NIH HHS/United States
- W81XWH-18-PH/TBIRP-LIMBIC under Awards No. W81XWH1920067 and W81XWH-13-2-0095/U.S. Department of Defense
- I01 RX003444/RX/RRD VA/United States
- UL1 RR025764/RR/NCRR NIH HHS/United States
- I01 RX003442/RX/RRD VA/United States
- I01 RX001774/RX/RRD VA/United States
- I01 CX002097/CX/CSRD VA/United States
- I01 CX002096/CX/CSRD VA/United States
- I01 CX001820/CX/CSRD VA/United States
- I01 RX002767/RX/RRD VA/United States
- I01 RX001135/RX/RRD VA/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
