

Developing and validation a prognostic model for predicting prognosis among synchronous colorectal cancers patients using combined log odds ratio of positive lymph nodes: a SEER database study
- PMID: 39587468
- PMCID: PMC11587701
- DOI: 10.1186/s12876-024-03393-7
Developing and validation a prognostic model for predicting prognosis among synchronous colorectal cancers patients using combined log odds ratio of positive lymph nodes: a SEER database study
Abstract
Purpose: The aim of the study is to identify risk factors for the prognosis and survival of synchronous colorectal cancer and to create and validate a functional Nomogram for predicting cancer-specific survival in patients with synchronous colorectal cancer.
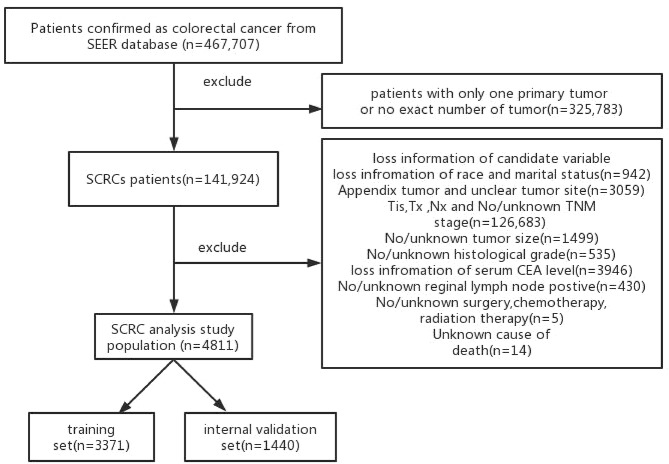
Methods: Synchronous colorectal cancers cases were retrieved from the Surveillance, Epidemiology, and End Results database retrospectively, then they were randomly divided into training (n = 3371) and internal validation (n = 1440) sets, and a set of 100 patients from our group was used as external validation. Risk factors for synchronous colorectal cancer were determined using univariate and multivariate Cox regression analyses, and two Nomograms were established to forecast the overall survival and cancer-specific survival, respectively. We assessed the Nomogram performance in terms of discrimination and calibration. Bootstrap resampling was used as an internal verification method, and we select external data from our hospital as independent validation sets.
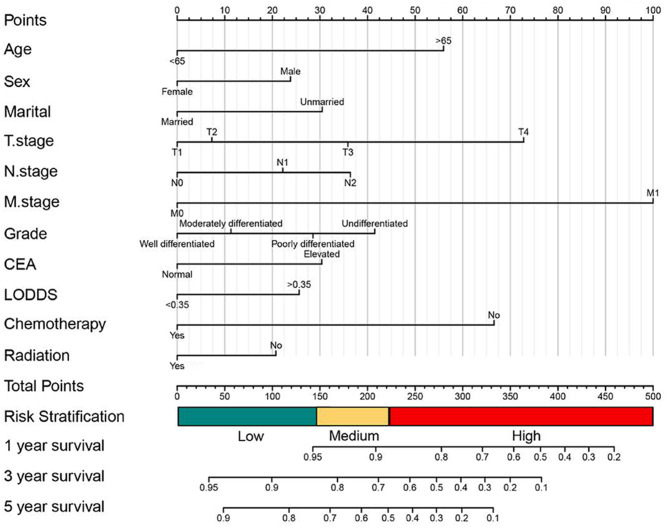
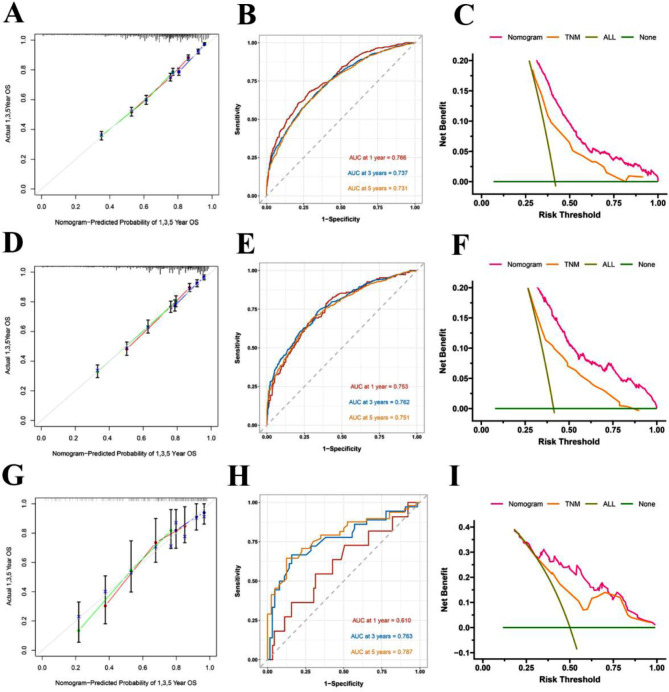
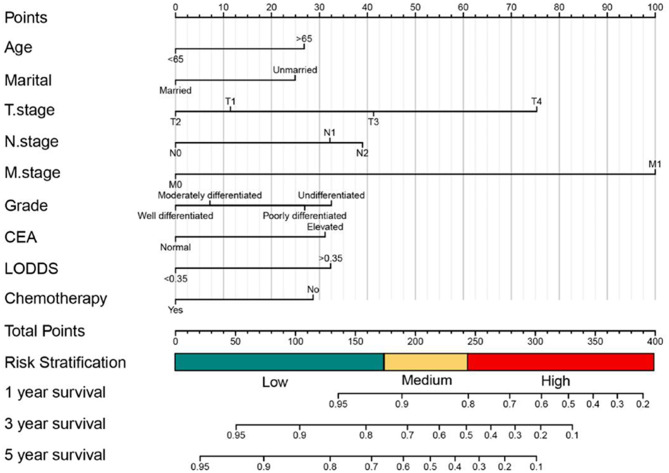
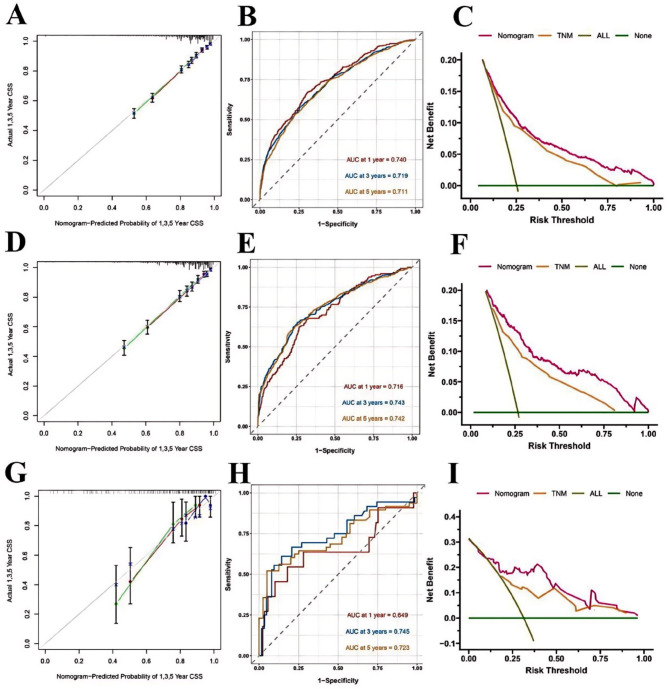
Results: Two Nomograms are established to predict the overall survival and cancer-specific survival. In OS Nomogram, sex, age, marital status, ttumor pathological grade, AJCC TNM stage, preoperative serum CEA level, LODDS, radiotherapy and chemotherapy were determined as prognostic factors. In CSS Nomogram, age and marital status, AJCC TNM stage, tumor pathological grade, preoperative serum CEA level, LODDS, radiotherapy and chemotherapy were determined as prognostic factors.The C-indexes for the forecast of overall survival were 0.70, and the C-index was 0.68 for the training and internal validation cohort, respectively. The C-indexes for the forecast of cancer-specific survival were 0.75, and the C-index was 0.74 for the training and internal validation cohort, respectively. The Nomogram calibration curves showed no significant deviation from the reference line, indicating a good level of calibration. Both C-index and calibration curves indicated noticeable performance of newly established Nomograms.
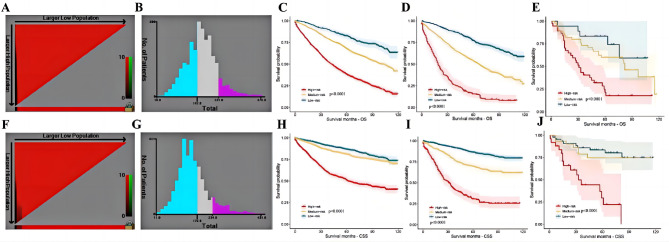
Conclusions: Those Nomograms with risk rating system can identify high risk patients who require more aggressive therapeutic intervention and longer and more frequent follow-up scheme, demonstrated prognostic efficiency.
Keywords: Cancer-specific survival; Nomogram; Overall survival; SEER; Synchronous colorectal cancers.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This retrospective study was approved by the institutional review board of Northern Jiangsu People’s Hospital. Written informed consent was obtained from all patients or their legal guardians. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Declaration of competing interest: Yue Ma, Bangquan Chen, Yayan Fu, Jun Ren and Daorong Wang declared that they have no conflict of interest.
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics 2022. CA: Cancer J Clin 72(1):7–33. 10.3322/caac.21708 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
