

Culture-negative sepsis may be a different entity from culture-positive sepsis: a prospective nationwide multicenter cohort study
- PMID: 39587586
- PMCID: PMC11587757
- DOI: 10.1186/s13054-024-05151-3
Culture-negative sepsis may be a different entity from culture-positive sepsis: a prospective nationwide multicenter cohort study
Abstract
Background: The distinction between culture-positive sepsis and culture-negative sepsis regarding clinical characteristics and outcomes remains contentious. We aimed to elucidate these differences using large-scale nationwide data.
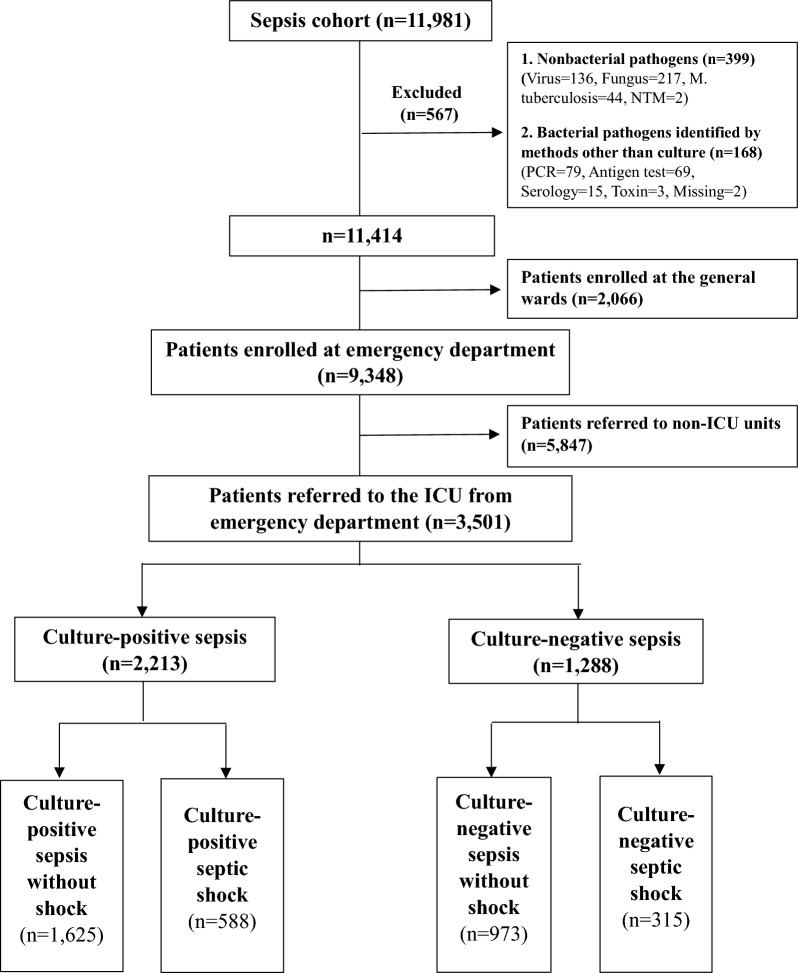
Methods: This prospective cohort study analyzed data from the Korean Sepsis Alliance registry, comprising 21 intensive care units (ICUs) across 20 hospitals from September 2019 to December 2021. Patients meeting the Sepsis-3 criteria were included.
Results: Among 11,981 sepsis patients, 3501 were analyzed, all of whom were referred to the ICU through the emergency department (mean age: 72 ± 13 years; 1976 [56%] males). Of these, 2213 (63%) were culture-positive sepsis and 1288 (37%) were culture-negative sepsis. Compared to the culture-positive sepsis group, the culture-negative sepsis group exhibited less severe illness, with lower Sequential Organ Failure Assessment scores and less deteriorated vital signs. While pulmonary-origin sepsis was common in both groups, culture-negative patients primarily presented with pulmonary infections and had a higher incidence of respiratory failure. In comparison to the culture-positive sepsis group, blood cultures and the administration of empirical antibiotics were performed less promptly in the culture-negative sepsis group. Patients with culture-negative sepsis also showed lower compliance with fluid resuscitation (98.4% vs. 96.9%, p = 0.038; culture-positive sepsis vs. culture-negative sepsis) and received vasopressors earlier (31.1% vs. 35.9%, p = 0.012). In-hospital mortality did not differ significantly between the two groups (31.6% vs. 34.9%, p = 0.073); however, in patients with septic shock, culture-negative sepsis had higher mortality rates (37.6% vs. 45.1%, p = 0.029). The apparent appropriateness of empirical antibiotics in the culture-negative septic shock was higher than that of the culture-positive septic shock (85.2% vs. 96.8%, p < 0.001). Culture-negativity independently predicted poor prognosis in septic shock patients (OR: 1.462, 95% CI [1.060-2.017], p = 0.021).
Conclusion: In patients with septic shock, culture-negativity was associated with increased mortality, despite the paradoxically higher appropriateness of empirical antibiotics than culture-positive patients. These contradictory findings suggest that the current criteria for determining the appropriateness of empirical antibiotic therapy may not be valid for culture-negative sepsis.
Keywords: Culture; Negative result; Sepsis; Shock, septic; Treatment outcome.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was approved by the Institutional Review Board of each participating hospital, including Inje University Sanggye Paik Hospital (Approval No. 2018-08-014-013), and the requirement for obtaining patient informed consent was waived because of the observational nature of the study. Additionally, the patient’s information was anonymized and de-identified prior to analysis. Consent for publication: Not applicable. Competing Interests: The authors declare that they have no competing interests.
Comment in
-
The elusive concept of appropriate antibiotic for septic patients when a pathogen is not detected by standard culture methods.Crit Care. 2025 Jan 6;29(1):7. doi: 10.1186/s13054-024-05240-3. Crit Care. 2025. PMID: 39762878 Free PMC article. No abstract available.
-
Pulmonary pathology in culture-negative sepsis: a potential confounder for sepsis treatment and research.Crit Care. 2025 Jan 24;29(1):44. doi: 10.1186/s13054-025-05267-0. Crit Care. 2025. PMID: 39856728 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
