

Cost-effectiveness of high flow nasal cannula therapy versus continuous positive airway pressure for non-invasive respiratory support in paediatric critical care
- PMID: 39587649
- PMCID: PMC11587665
- DOI: 10.1186/s13054-024-05148-y
Cost-effectiveness of high flow nasal cannula therapy versus continuous positive airway pressure for non-invasive respiratory support in paediatric critical care
Abstract
Background: High flow nasal cannula therapy (HFNC) and continuous positive airway pressure (CPAP) are two widely used modes of non-invasive respiratory support in paediatric critical care units. The FIRST-ABC randomised controlled trials (RCTs) evaluated the clinical and cost-effectiveness of HFNC compared with CPAP in two distinct critical care populations: acutely ill children ('step-up' RCT) and extubated children ('step-down' RCT). Clinical effectiveness findings (time to liberation from all forms of respiratory support) showed that HFNC was non-inferior to CPAP in the step-up RCT, but failed to meet non-inferiority criteria in the step-down RCT. This study evaluates the cost-effectiveness of HFNC versus CPAP.
Methods: All-cause mortality, health-related Quality of Life (HrQoL), and costs up to six months were reported using FIRST-ABC RCTs data. HrQoL was measured with the age-appropriate Paediatric Quality of Life Generic Core Scales questionnaire and mapped onto the Child Health Utility 9D index score at six months. Quality-Adjusted Life Years (QALYs) were estimated by combining HrQoL with mortality. Costs at six months were calculated by measuring and valuing healthcare resources used in paediatric critical care units, general medical wards and wider health service. The cost-effectiveness analysis used regression methods to report the cost-effectiveness of HFNC versus CPAP at six months and summarised the uncertainties around the incremental cost-effectiveness results.
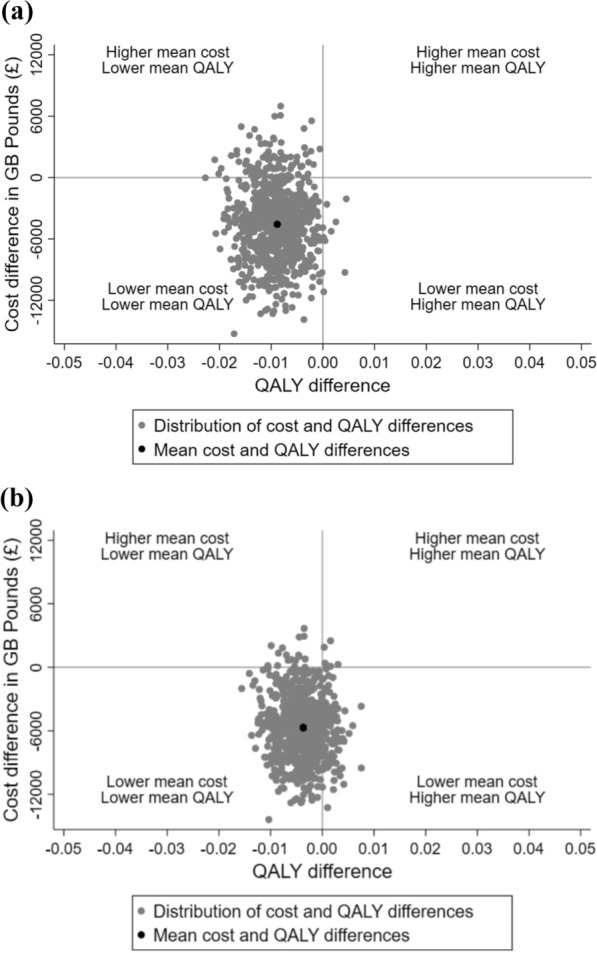
Results: In both RCTs, the incremental QALYs at six months were similar between the randomised groups. The estimated incremental cost at six months was - £4565 (95% CI - £11,499 to £2368) and - £5702 (95% CI - £11,328 to - £75) for step-down and step-up RCT, respectively. The incremental net benefits of HFNC versus CPAP in step-down RCT and step-up RCT were £4388 (95% CI - £2551 to £11,327) and £5628 (95% CI - £8 to £11,264) respectively. The cost-effectiveness results were surrounded by considerable uncertainties. The results were similar across most pre-specified subgroups, and the base case results were robust to alternative assumptions.
Conclusions: HFNC compared to CPAP as non-invasive respiratory support for critically-ill children in paediatric critical care units reduces mean costs and is relatively cost-effective overall and for key subgroups, although there is considerable statistical uncertainty surrounding this result.
Keywords: Continuous positive airway pressure; Cost-effectiveness; High-flow nasal cannula; Incremental net benefit; Non-invasive respiratory support; Paediatric critical care.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical approval and consent to participate: The FIRST-ABC master protocol was approved by the East of England–Cambridge South Research Ethics Committee (19/EE/0185) and the UK Health Research Authority (IRAS 260536). The trial was registered with the International Standard Randomised Controlled Trial Number (ISRCTN) Registry (ISRCTN60048867). Written informed consent was obtained from parents/legal guardians of each trial participant. Consent for publication: Not applicable. Competing interests: The authors report funding from the National Institute for Health and Social Care Research (NIHR) Health Technology Assessment Programme to their institutions for the work presented in the manuscript. KR is Director of the NIHR Health and Social Care Delivery Research Programme.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
