

Catheter ablation of atrial fibrillation in women with heart failure with preserved ejection fraction
- PMID: 39588067
- PMCID: PMC11586357
- DOI: 10.3389/fcvm.2024.1463815
Catheter ablation of atrial fibrillation in women with heart failure with preserved ejection fraction
Abstract
Background: Heart failure with preserved ejection fraction (HFpEF) and atrial fibrillation (AF) often coincide. Female sex is associated with both increased prevalence of HFpEF and reduced therapeutic efficacy of catheter ablation of AF. This sub-analysis of the previously published AFFECT-study evaluates outcome after cryoballoon-ablation in women with and without HFpEF.
Methods: One-hundred-and-two patients (LVEF ≥ 50%) scheduled for cryoballoon-ablation of AF were prospectively enrolled. Forty-two were female. Comprehensive baseline assessment included echocardiography, stress echocardiography, six-minute-walk-test, biomarker- and quality-of-life-assessment (QoL, SF-36), and was repeated at follow-up ≥12 months after AF-ablation. Baseline parameters, procedural characteristics and outcome after AF-ablation were compared between women with and without HFpEF.
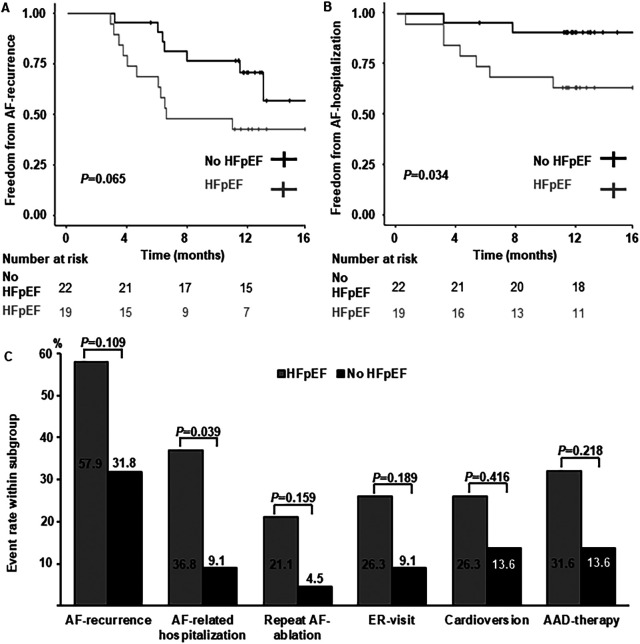
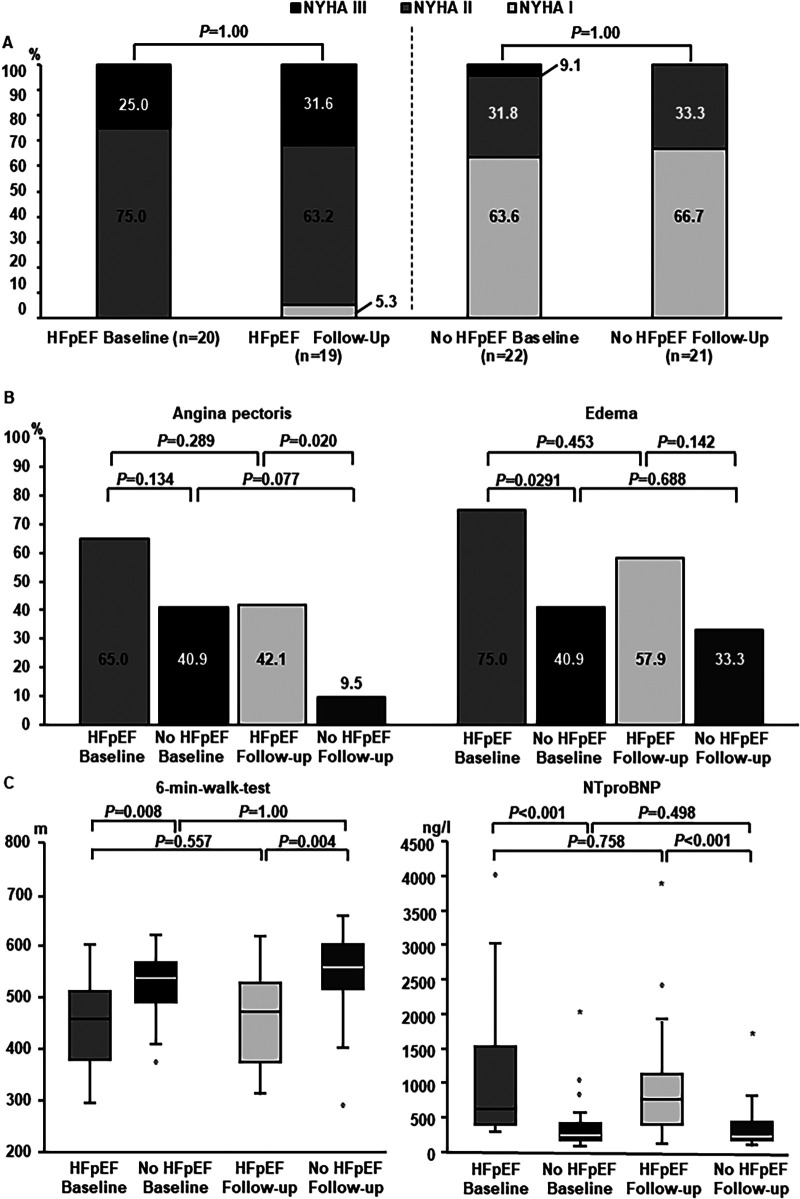
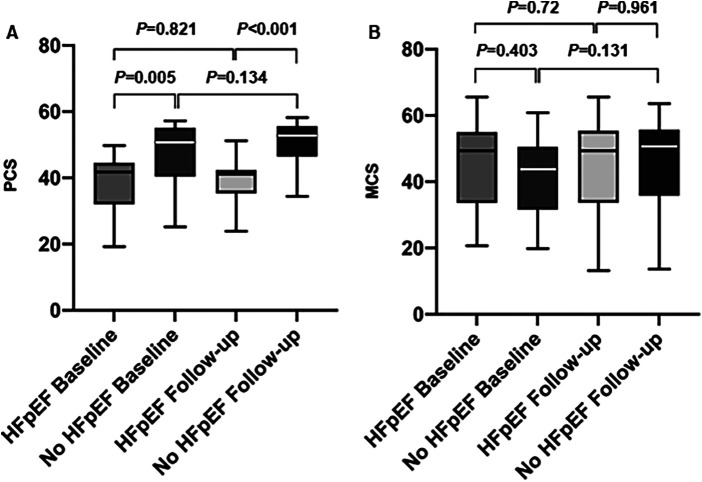
Results: Women with HFpEF (n = 20) were characterized by higher median left atrial volume index (35.8 ml/m2 vs. 25.8 ml/m2, P < 0.001), left ventricular hypertrophy (median left ventricular mass index: 92.0 g/m2 vs. 83.0 g/m2, P = 0.027), reduced distance in the 6-min-walk-test (median: 453 m vs. 527 m, P = 0.008) and higher left atrial pressures (median: 14.0 mmHg vs.9.5 mmHg, P = 0.008) compared to women without HFpEF (n = 21). During follow-up, HFpEF-patients more often experienced AF-related re-hospitalization (36.8% vs. 9.1%, P = 0.039) and numerically higher AF-recurrence-rates (57.9% vs. 31.1%, P = 0.109). There was no significant improvement of heart failure-related symptoms, echocardiographic parameters and cardiac biomarkers levels. QoL showed no significant improvement in both subgroups. Women with HFpEF still exhibited a lower SF-36 Physical Component Summary Score vs. women without HFpEF (median: 41.2 vs. 52.1, P < 0.001).
Conclusion: Women with HFpEF constitute a distinct subgroup with high rates of AF-related events after AF-ablation, and persistence of both symptoms and functional hallmarks of HFpEF. Consideration of sex-specific cardiac co-morbidities is crucial for personalization and optimization of AF-therapy.
Clinical trial registration: ClinicalTrials.gov Identifier NCT05603611.
Keywords: HFpEF; atrial fibrillation; catheter ablation; pulmonary vein isolation; women.
© 2024 Zylla, Leiner, Rahm, Hoffmann, Lugenbiel, Schweizer, Mages, Mereles, Kieser, Scholz, Katus, Frey and Thomas.
Conflict of interest statement
MZ reports lecture fees/honoraria, educational grants and travel support by Medtronic, Boston Scientific, Bayer Vital, ZOLL CMS and Pfizer. A-KR reports educational grants and travel support by Medtronic, Biosense Webster and Boston Scientific. PL reports receiving lecture fees/honoraria from Bayer Vital, Boston Scientific, Biosense Webster, Pfizer and Medtronic. NF reports receiving lecture fees/honoraria from AstraZeneca, Bayer Vital, Boehringer Ingelheim Pharma, Daiichi Sankyo, Novartis and Pfizer Pharma, none of which related to the content of this manuscript. DT reports receiving lecture fees/honoraria from AstraZeneca, Bayer Vital, Boehringer Ingelheim Pharma, Bristol-Myers Squibb, Daiichi Sankyo, Medtronic, Pfizer Pharma, Sanofi-Aventis, St. Jude Medical and ZOLL CMS. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2021) 42(5):373–498. 10.1093/eurheartj/ehaa612 - DOI - PubMed
-
- Tzeis S, Gerstenfeld EP, Kalman J, Saad E, Shamloo AS, Andrade JG, et al. 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation. EP Europace. (2024) 26(4):euae043. 10.1093/europace/euae043 - DOI - PMC - PubMed
-
- Linde C, Bongiorni MG, Birgersdotter-Green U, Curtis AB, Deisenhofer I, Furokawa T, et al. Sex differences in cardiac arrhythmia: a consensus document of the European Heart Rhythm Association, endorsed by the Heart Rhythm Society and Asia Pacific Heart Rhythm Society. Europace. (2018) 20(10):1565. 10.1093/europace/euy067 - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical