

Our Experience in Treating Infantile Hemangioma: Prognostic Factors for Relapse After Propranolol Discontinuation
- PMID: 39589452
- PMCID: PMC11782296
- DOI: 10.1007/s12325-024-03017-2
Our Experience in Treating Infantile Hemangioma: Prognostic Factors for Relapse After Propranolol Discontinuation
Abstract
Introduction: Infantile hemangioma (IH) is a common benign tumor in infants. While most cases exhibit a self-limiting nature, some require medical treatment to avoid complications. Propranolol is the first-line therapy for IH, it has a high success rate, and is safe to use. Unfortunately, some patients might experience rebound growth after propranolol discontinuation. Currently, it is unclear which factors predict this phenomenon. This study aimed to identify factors affecting the rebound growth of IH after propranolol cessation. We also aimed to identify predictors for an excellent response to oral propranolol.
Methods: We performed a retrospective cohort study using clinical data from all patients referred to our clinic with IH and placed on systemic oral propranolol between January 2009 to December 2023 in the dermatology outpatient clinic of Rambam Healthcare Campus.
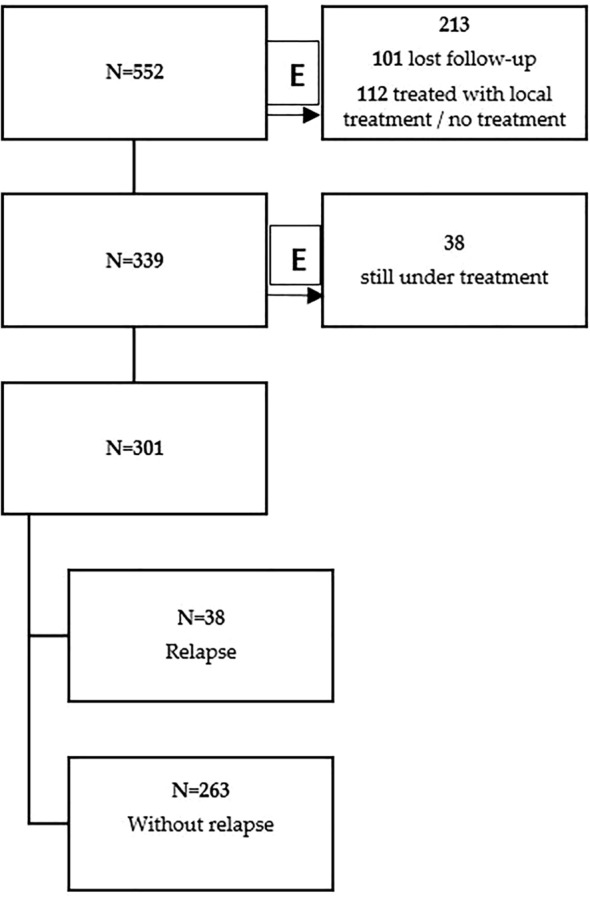
Results: Out of a total of 552 patients with IH, 301 received oral propranolol for at least 6 months. A relapse phenomenon was observed in 38 (12.6%) patients. We found a significant association between limb involvement and the least likelihood of hemangioma rebound (p < 0.001). An excellent response to oral propranolol was observed in 57.8% of patients. Younger age at initiation of oral propranolol was associated with an excellent response (p = 0.015). Also, IHs located on the limbs (67) showed a higher rate of excellent response to oral propranolol compared to other anatomical sites (p = 0.02). Interestingly, patients who were treated with a dose of 2 mg/kg/day were associated with excellent response to treatment (p = 0.007).
Conclusions: IHs located on the limbs demonstrated less rebound growth and a better treatment response. When oral propranolol was initiated earlier or when the target dose was 2 mg/kg/day, there was a higher rate of excellent response to treatment.
Keywords: Infantile hemangioma; Prognostic factors; Propranolol; Rebound; Relapse.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: Hiba Zaaroura, Afik Tibi, Emily Avitan-Hersh, and Ziad Khamaysi declare that they have no competing interests. Ethical Approval: Because of the retrospective nature of the study, we did not obtain consent from the patients, but we did obtain consent to publish. The study was approved by the local institutional review board committee—approval number 0624-23.
Figures

References
-
- Pam N, Kridin K, Khamaysi Z. Propranolol for infantile hemangioma: evaluating efficacy and predictors of response and rebound growth. Dermatol Ther. 2021;34(3):e14936. - PubMed
-
- Kilcline C, Frieden IJ. Infantile hemangiomas: how common are they? A systematic review of the medical literature. Pediatr Dermatol. 2008;25(2):168–73. - PubMed
-
- Krowchuk DP, Frieden IJ, Mancini AJ, et al. Clinical practice guideline for the management of infantile hemangiomas. Pediatrics. 2019. 10.1542/peds.2018-3475. - PubMed
-
- Kridin K, Pam N, Bergman R, Khamaysi Z. Oral propranolol administration is effective for infantile hemangioma in late infancy: a retrospective cohort study. Dermatol Ther. 2020. 10.1111/dth.13331. - PubMed
-
- Bruckner AL, Frieden IJ. Hemangiomas of infancy. J Am Acad Dermatol. 2003. 10.1067/mjd.2003.200. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
