

Different Proteins as Biomarkers for Sac Shrinkage After Endovascular Aortic Repair of Abdominal Aortic Aneurysms
- PMID: 39590217
- PMCID: PMC11594911
- DOI: 10.3390/jcdd11110374
Different Proteins as Biomarkers for Sac Shrinkage After Endovascular Aortic Repair of Abdominal Aortic Aneurysms
Abstract
Background: This study aims to identify circulating biomarkers by using proteomic analysis associated with sac shrinkage or expansion in patients undergoing endovascular aneurysm repair (EVAR) for abdominal aortic aneurysms (AAAs).
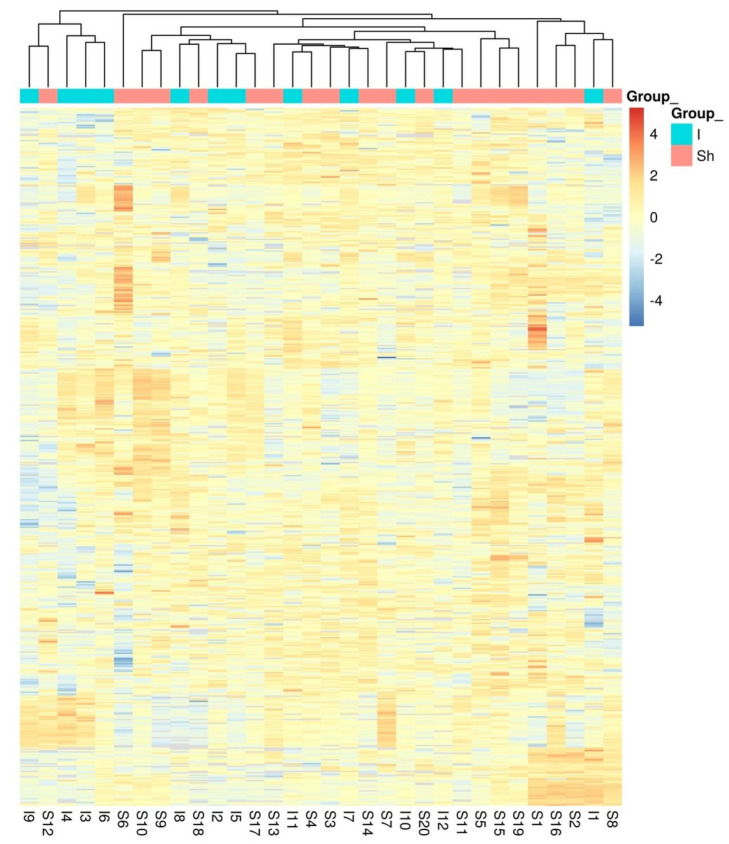
Methods: Plasma samples were analysed from 32 patients treated with EVAR between 10/2009 and 10/2020. Patients were divided into two groups based on postoperative sac behaviour: sac shrinkage (≥5 mm reduction) and no shrinkage (stabilisation or expansion). Proteomic analysis was performed using high-resolution liquid chromatography-tandem mass spectrometry (LC-MS/MS), with abundant protein depletion to enhance the detection of low-abundant proteins.
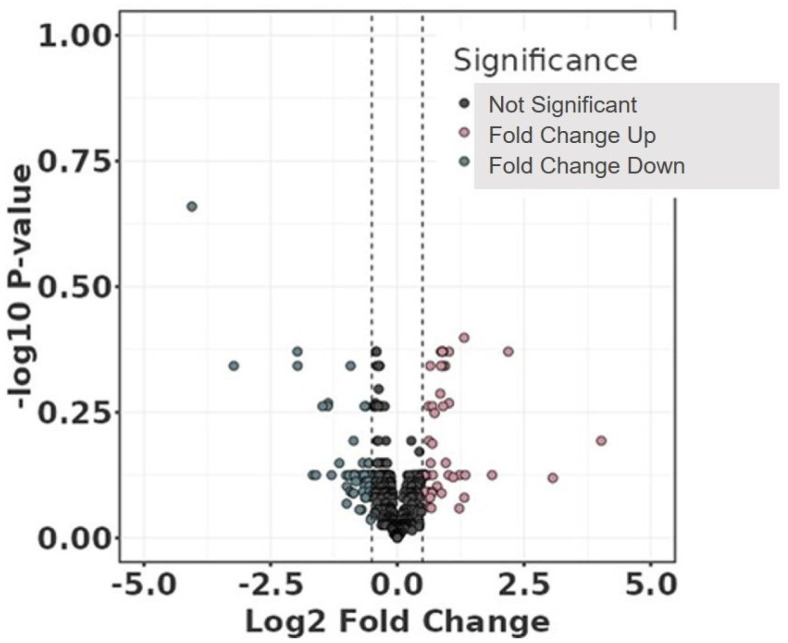
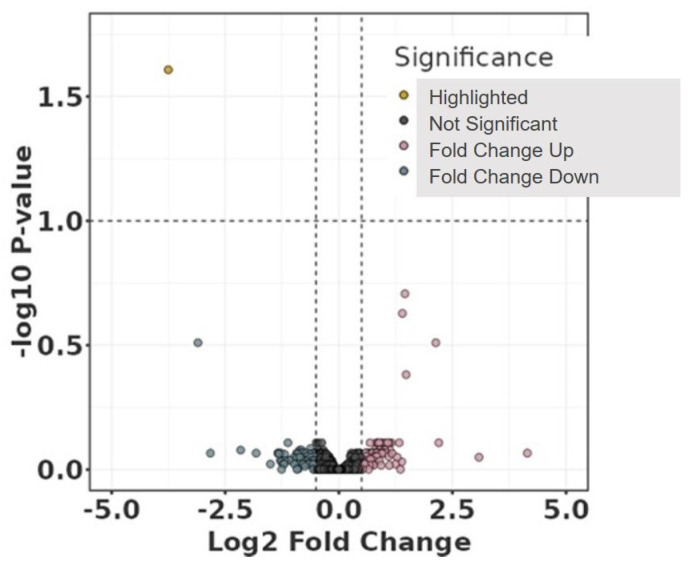
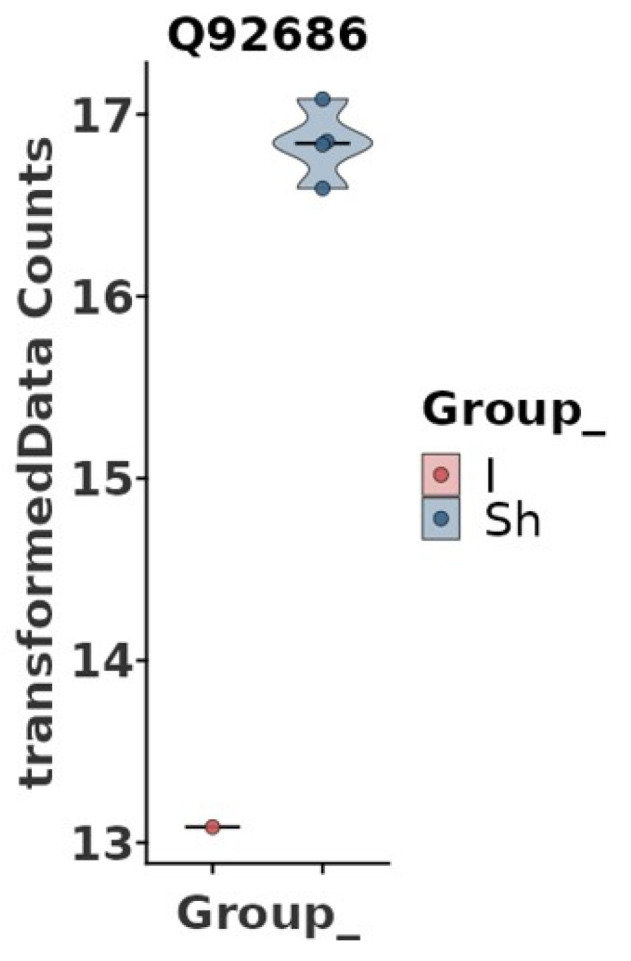
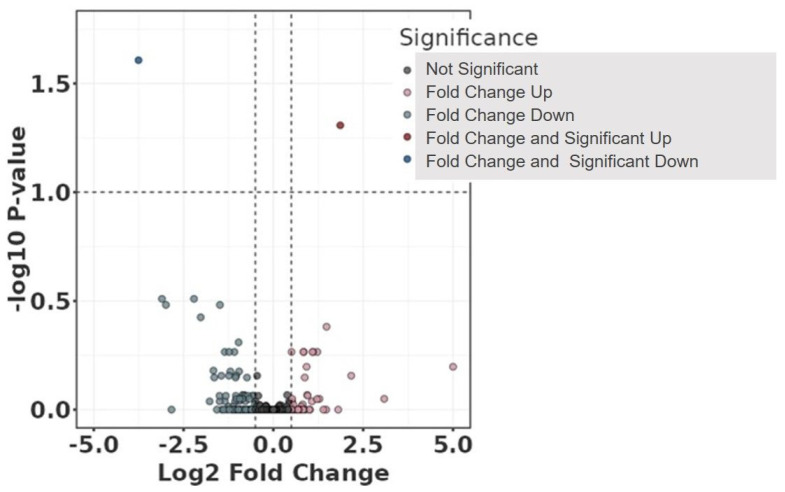
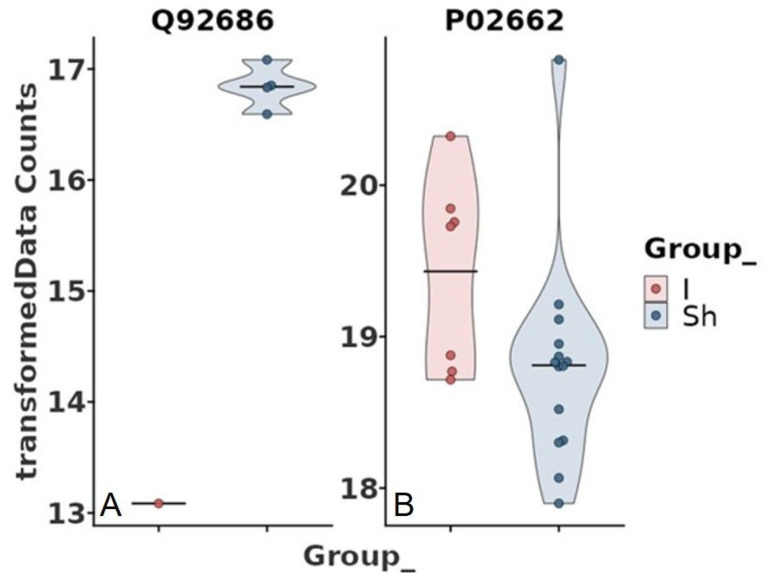
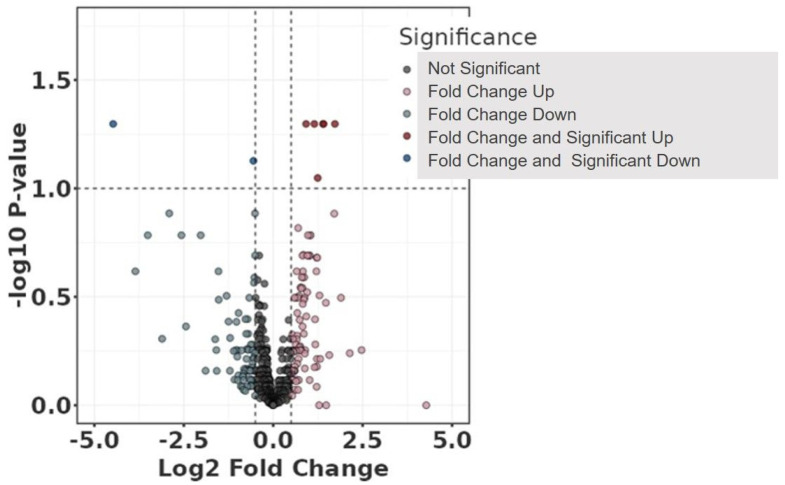
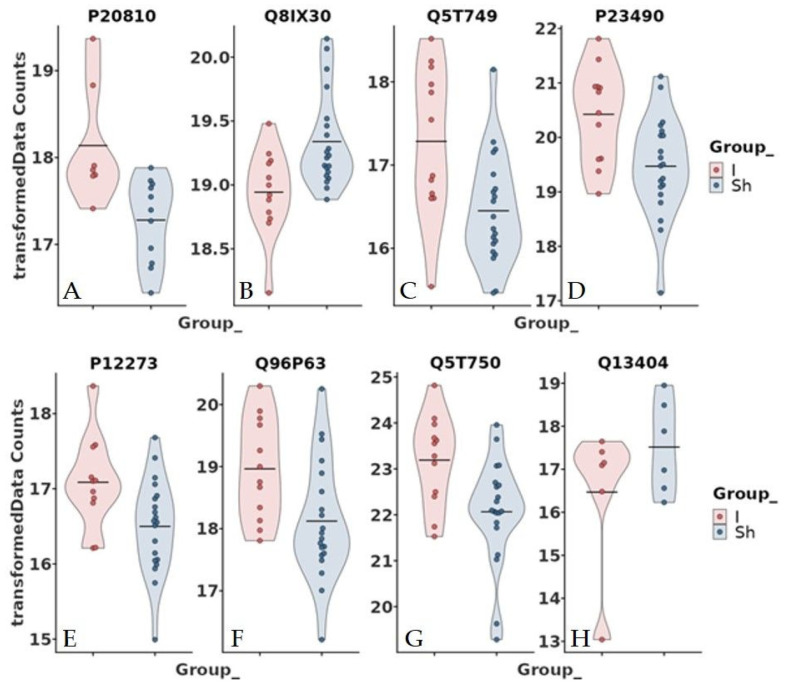
Results: Of the 32 patients, 20 exhibited sac shrinkage, and 12 showed no shrinkage. Proteomic analysis identified 632 proteins, with significant differential abundance observed after adjusting for relevant clinical parameters. Notably, neurogranin (NRGN) levels were significantly associated with hypertension and smoking, while casein alpha S1 (CSN1S1) levels varied with statin use. Differentially abundant proteins related to aortic diameter included calpastatin, SCUBE3, and ubiquitin-conjugating enzyme E2, among others.
Conclusions: Proteomic profiling revealed distinct biomarker patterns associated with sac behaviour in EVAR-treated AAA patients. These findings suggest potential therapeutic targets for enhancing EVAR outcomes and underscore the need for further investigation into the biological mechanisms underlying aneurysm sac shrinkage and stability.
Keywords: SCUBE3; aneurysm diameter; calpastatin; casein alpha S1; endovascular aneurysm repair; neurogranin; proteomics; ubiquitin-conjugating enzyme E2.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Meuli L., Menges A.-L., Steigmiller K., Kuehnl A., Reutersberg B., Held U., Zimmermann A. Hospital Incidence and Mortality of Patients Treated for Abdominal Aortic Aneurysms in Switzerland—A Secondary Analysis of Swiss DRG Statistics Data. Swiss Med. Wkly. 2022;152:w30191. doi: 10.4414/SMW.2022.w30191. - DOI - PubMed
-
- Lederle F.A., Freischlag J.A., Kyriakides T.C., Matsumura J.S., Padberg F.T.J., Kohler T.R., Kougias P., Jean-Claude J.M., Cikrit D.F., Swanson K.M. Long-Term Comparison of Endovascular and Open Repair of Abdominal Aortic Aneurysm. N. Engl. J. Med. 2012;367:1988–1997. doi: 10.1056/NEJMoa1207481. - DOI - PubMed
-
- O’Donnell T.F.X., Deery S.E., Boitano L.T., Siracuse J.J., Schermerhorn M.L., Scali S.T., Schanzer A., Lancaster R.T., Patel V.I. Aneurysm Sac Failure to Regress after Endovascular Aneurysm Repair Is Associated with Lower Long-Term Survival. J. Vasc. Surg. 2019;69:414–422. doi: 10.1016/j.jvs.2018.04.050. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
