

Innominate Artery Translocation with Hemiarch Replacement Strategy for Acute Type A Aortic Dissection: a Single-Center Study
- PMID: 39592007
- PMCID: PMC11879489
- DOI: 10.1055/s-0044-1795129
Innominate Artery Translocation with Hemiarch Replacement Strategy for Acute Type A Aortic Dissection: a Single-Center Study
Abstract
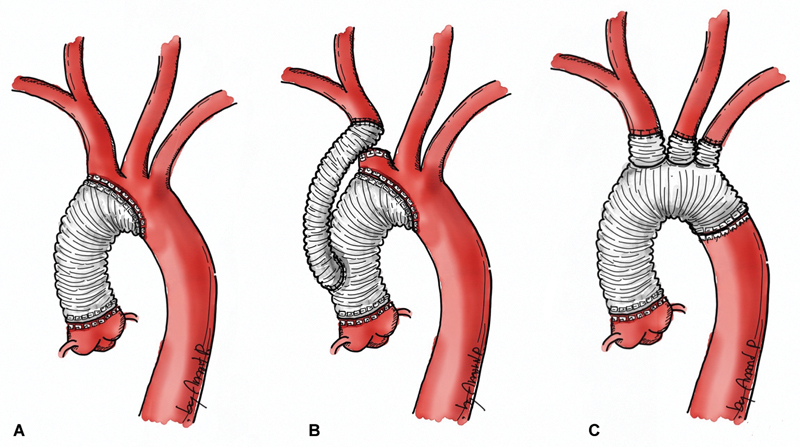
Background: Aggressive surgical methods for acute type A aortic dissection (ATAD) can cause extended operating times and postoperative complications. less extensive techniques may increase the risk of needing further aortic reintervention. To prevent the need for extensive aortic arch surgery and subsequent re-sternotomy, hemiarch replacement (HAR) with innominate artery (a.) translocation is performed to create a suitable proximal landing zone for future endovascular repair.
Methods: Retrospective study of 112 patients with ATAD who underwent aortic surgery from January 2009 to December 2020. Forty-one patients underwent HAR with innominate artery translocation, 16 underwent total arch replacement (TAR), and 55 underwent only HAR. Multivariable Cox regression and logistic regression analyses were used to study the outcomes and risk factors.
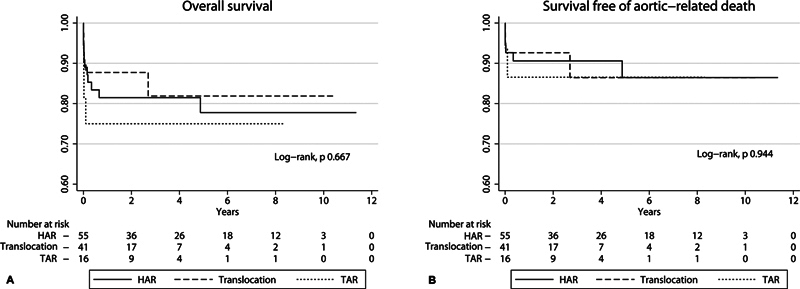
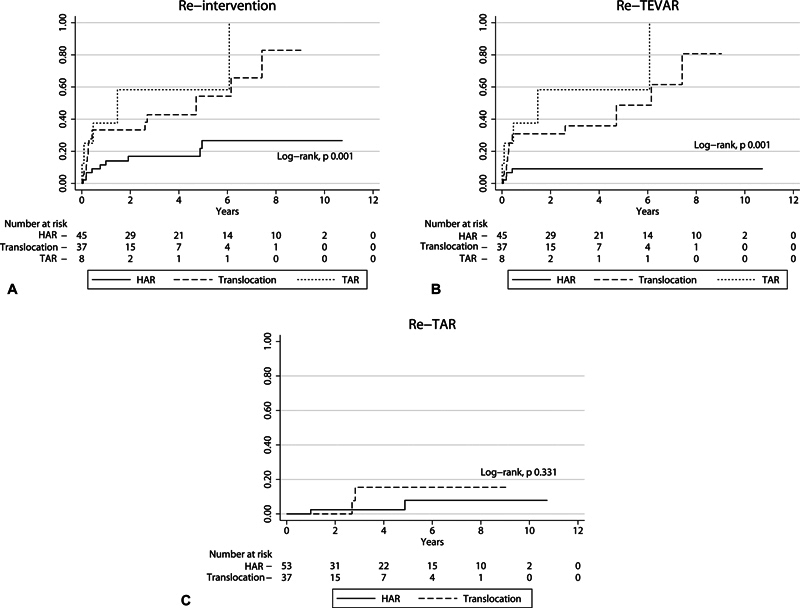
Results: The TAR group had a higher incidence of postoperative acute kidney injury. The overall mortality rate of the TAR group was 25%, compared with 20% in the HAR group and 14.6% in the translocation group. The 5-year overall survival rates for the groups were 81.9%, 75.0%, and 77.7%, respectively. False lumen thrombosis at the aortic arch and descending aorta level were factors associated with reduced mortality in both univariable and multivariable analyses. The translocation group had a significantly higher reintervention rate of 41.5% compared with the TAR and HAR groups, with rates of 31.3% and 16.4%, respectively. The median reintervention time for the translocation group was 4.72 years.
Conclusion: Despite the innominate translocation technique having a higher reintervention rate, it had similar mortality outcomes to HAR and TAR. Thus, it could be a more convenient option for reintervention, including creating a proximal landing zone, which could benefit patients needing endovascular repair.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
None declared.
Figures
Similar articles
-
One-Stage Hybrid Total Aortic Arch and Descending Thoracic Aortic Repair is a Safe and Secure Procedure With Less Postoperative Complications for Extended Aortic Arch Aneurysms.J Endovasc Ther. 2022 Apr;29(2):204-214. doi: 10.1177/15266028211047954. Epub 2021 Sep 28. J Endovasc Ther. 2022. PMID: 34581224
-
Safety and arch complications after hemiarch versus total arch replacement with stented elephant trunk in acute type 1 dissection: Is a stent graft always beneficial?JTCVS Open. 2022 Jun 25;11:14-22. doi: 10.1016/j.xjon.2022.06.014. eCollection 2022 Sep. JTCVS Open. 2022. PMID: 36172444 Free PMC article.
-
Outcomes of two-stage type II hybrid aortic arch repair in elderly patients with acute type A aortic dissection.Sci Rep. 2024 Jan 17;14(1):1522. doi: 10.1038/s41598-024-51784-3. Sci Rep. 2024. PMID: 38233509 Free PMC article.
-
Is extended arch replacement justified for acute type A aortic dissection?Interact Cardiovasc Thorac Surg. 2015 Jan;20(1):120-6. doi: 10.1093/icvts/ivu323. Epub 2014 Oct 3. Interact Cardiovasc Thorac Surg. 2015. PMID: 25281706 Review.
-
The frozen elephant trunk: seeking a more definitive treatment for acute type A aortic dissection.Eur J Cardiothorac Surg. 2024 May 3;65(5):ezae176. doi: 10.1093/ejcts/ezae176. Eur J Cardiothorac Surg. 2024. PMID: 38676575 Review.
References
-
- Rylski B, Beyersdorf F, Kari F A, Schlosser J, Blanke P, Siepe M.Acute type A aortic dissection extending beyond ascending aorta: limited or extensive distal repair J Thorac Cardiovasc Surg 201414803949–954., discussion 954 - PubMed
-
- Shi E, Gu T, Yu Y et al.Simplified total arch repair with a stented graft for acute DeBakey type I dissection. J Thorac Cardiovasc Surg. 2014;148(05):2147–2154. - PubMed
-
- Shi E, Gu T, Yu Y et al.Early and midterm outcomes of hemiarch replacement combined with stented elephant trunk in the management of acute DeBakey type I aortic dissection: comparison with total arch replacement. J Thorac Cardiovasc Surg. 2014;148(05):2125–2131. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous