

Effect of a driving pressure-limiting strategy for patients with acute respiratory distress syndrome secondary to community-acquired pneumonia: the STAMINA randomised clinical trial
- PMID: 39592365
- PMCID: PMC11867071
- DOI: 10.1016/j.bja.2024.10.012
Effect of a driving pressure-limiting strategy for patients with acute respiratory distress syndrome secondary to community-acquired pneumonia: the STAMINA randomised clinical trial
Abstract
Background: This study aimed to assess whether a driving pressure-limiting strategy based on positive end-expiratory pressure (PEEP) titration according to best respiratory system compliance and tidal volume adjustment increases the number of ventilator-free days within 28 days in patients with moderate to severe acute respiratory distress syndrome (ARDS).
Methods: This is a multi-centre, randomised trial, enrolling adults with moderate to severe ARDS secondary to community-acquired pneumonia. Patients were randomised to a driving pressure-limiting strategy or low PEEP strategy based on a PEEP:FiO2 table. All patients received volume assist-control mode until day 3 or when considered ready for spontaneous modes of ventilation. The primary outcome was ventilator-free days within 28 days. Secondary outcomes were in-hospital and intensive care unit mortality at 90 days.
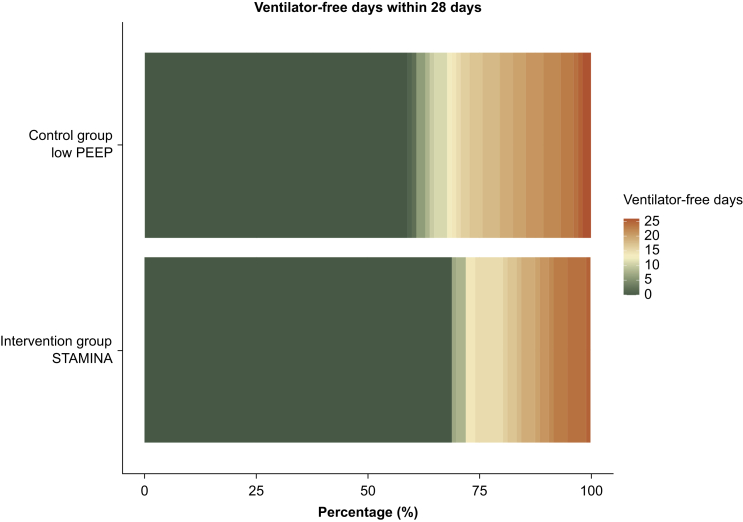
Results: The trial was stopped because of recruitment fatigue after 214 patients were randomised. In total, 198 patients (n=96 intervention group, n=102 control group) were available for analysis (median age 63 yr, [interquartile range 47-73 yr]; 36% were women). The mean difference in driving pressure up to day 3 between the intervention and control groups was -0.7 cm H2O (95% confidence interval -1.4 to -0.1 cm H2O). Mean ventilator-free days were 6 (sd 9) in the driving pressure-limiting strategy group and 7 (9) in the control group (proportional odds ratio 0.72, 95% confidence interval 0.39-1.32; P=0.28). There were no significant differences regarding secondary outcomes.
Conclusions: In patients with moderate to severe ARDS secondary to community-acquired pneumonia, a driving pressure-limiting strategy did not increase the number of ventilator-free days compared with a standard low PEEP strategy within 28 days.
Clinical trial registration: NCT04972318.
Keywords: acute respiratory distress syndrome; driving pressure; positive end-expiratory pressure; tidal volume; ventilator-induced lung injury.
Copyright © 2024 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interest The authors declare that they have no conflicts of interest.
Figures


References
-
- Bellani G., Laffey J.G., Pham T., et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315:788–800. - PubMed
-
- Gattinoni L., Marini J.J., Pesenti A., Quintel M., Mancebo J., Brochard L. The “baby lung” became an adult. Intensive Care Med. 2016;42:663–673. - PubMed
-
- Fan E., Brodie D., Slutsky A.S. Acute respiratory distress syndrome: advances in diagnosis and treatment. JAMA. 2018;319:698–710. - PubMed
-
- Amato M.B., Meade M.O., Slutsky A.S., et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372:747–755. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
