

Gucy1α1 specifically marks kidney, heart, lung and liver fibroblasts
- PMID: 39592775
- PMCID: PMC11599588
- DOI: 10.1038/s41598-024-80930-0
Gucy1α1 specifically marks kidney, heart, lung and liver fibroblasts
Abstract
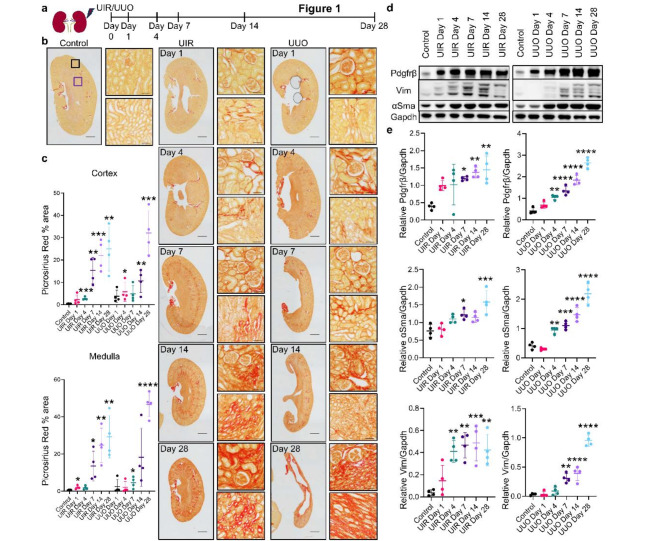
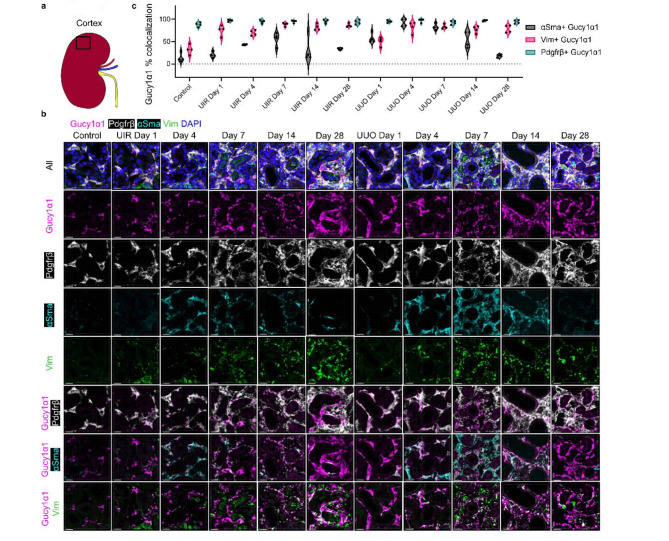
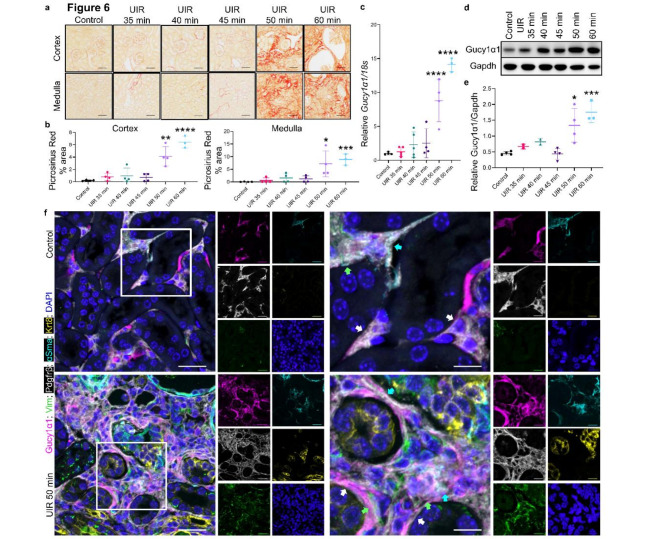
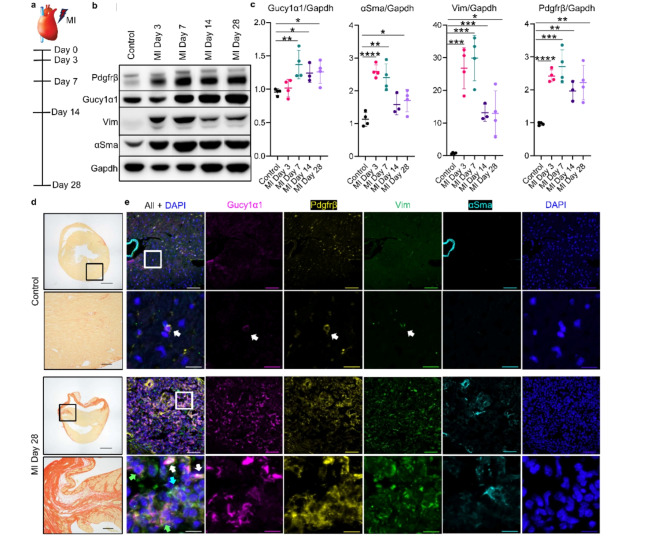
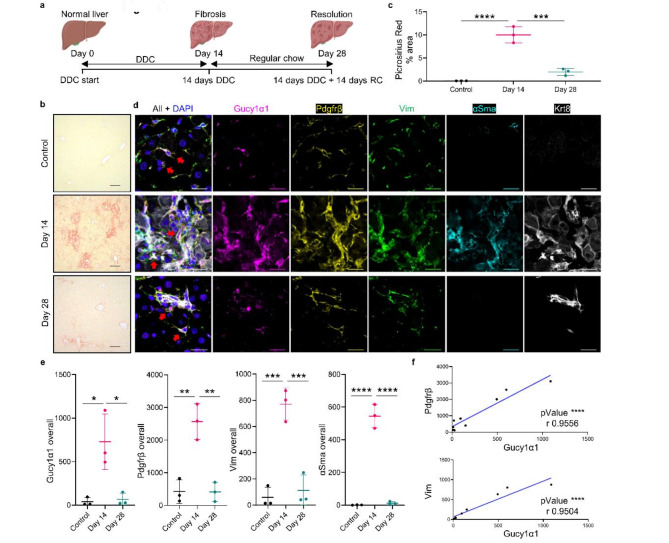
Fibrosis is a common outcome of numerous pathologies, including chronic kidney disease (CKD), a progressive renal function deterioration. Current approaches to target activated fibroblasts, key effector contributors to fibrotic tissue remodeling, lack specificity. Here, we report Gucy1α1 as a specific kidney fibroblast marker. Gucy1α1 levels significantly increased over the course of two clinically relevant murine CKD models and directly correlated with established fibrosis markers. Immunofluorescent (IF) imaging showed that Gucy1α1 comprehensively labelled cortical and medullary quiescent and activated fibroblasts in the control kidney and throughout injury progression, respectively. Unlike traditionally used markers platelet derived growth factor receptor beta (Pdgfrβ) and vimentin (Vim), Gucy1α1 did not overlap with off-target populations such as podocytes. Notably, Gucy1α1 labelled kidney fibroblasts in both male and female mice. Furthermore, we observed elevated GUCY1α1 expression in the human fibrotic kidney and lung. Studies in the murine models of cardiac and liver fibrosis revealed Gucy1α1 elevation in activated Pdgfrβ-, Vim- and alpha smooth muscle actin (αSma)-expressing fibroblasts paralleling injury progression and resolution. Overall, we demonstrate Gucy1α1 as an exclusive fibroblast marker in both sexes. Due to its multiorgan translational potential, GUCY1α1 might provide a novel promising strategy to specifically target and mechanistically examine fibroblasts.
Keywords: CKD; Kidney fibrosis; Multiorgan fibroblast marker.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures



Update of
-
Gucy1α1 specifically marks kidney, heart, lung and liver fibroblasts.bioRxiv [Preprint]. 2024 May 15:2024.05.15.594404. doi: 10.1101/2024.05.15.594404. bioRxiv. 2024. Update in: Sci Rep. 2024 Nov 26;14(1):29307. doi: 10.1038/s41598-024-80930-0. PMID: 38798483 Free PMC article. Updated. Preprint.
-
Gucy1α1 specifically marks kidney, heart, lung and liver fibroblasts.Res Sq [Preprint]. 2024 Aug 17:rs.3.rs-4746078. doi: 10.21203/rs.3.rs-4746078/v1. Res Sq. 2024. Update in: Sci Rep. 2024 Nov 26;14(1):29307. doi: 10.1038/s41598-024-80930-0. PMID: 39184103 Free PMC article. Updated. Preprint.
References
-
- Yamashita, N. & Kramann, R. Mechanisms of kidney fibrosis and routes towards therapy. Trends Endocrinol. Metab.35, 31–48. 10.1016/j.tem.2023.09.001 (2024). - PubMed
-
- Li, L., Fu, H. & Liu, Y. The fibrogenic niche in kidney fibrosis: Components and mechanisms. Nat. Rev. Nephrol.18, 545–557. 10.1038/s41581-022-00590-z (2022). - PubMed
-
- Nath, K. A. Tubulointerstitial changes as a major determinant in the progression of renal damage. Am. J. Kidney Dis.20, 1–17. 10.1016/s0272-6386(12)80312-x (1992). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
