

Genetic basis of early onset and progression of type 2 diabetes in South Asians
- PMID: 39592779
- PMCID: PMC11750703
- DOI: 10.1038/s41591-024-03317-8
Genetic basis of early onset and progression of type 2 diabetes in South Asians
Abstract
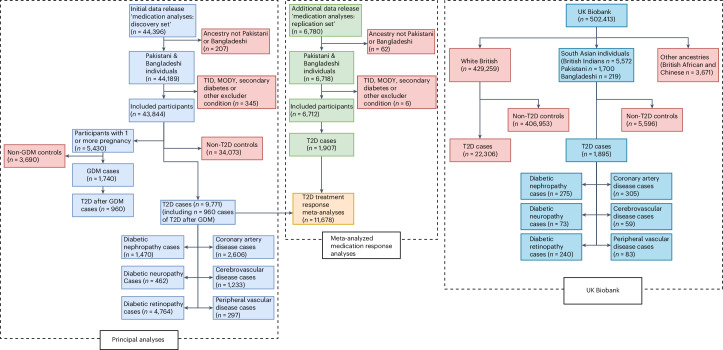
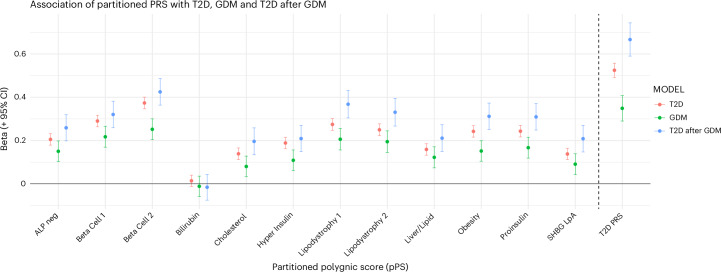
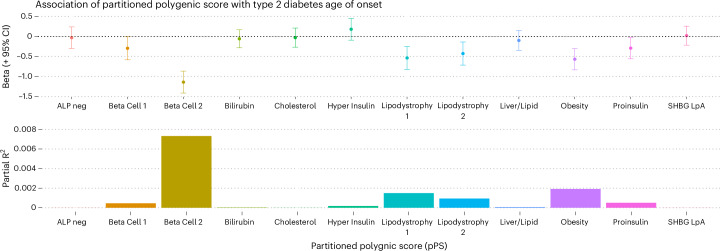
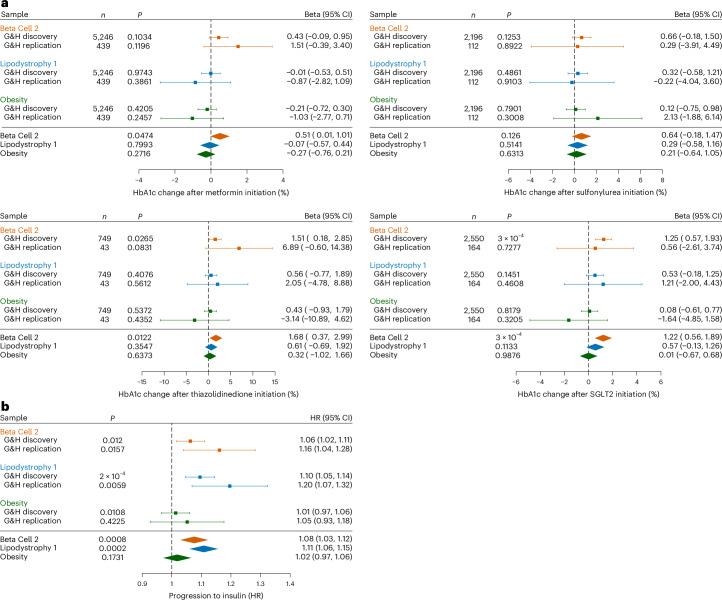
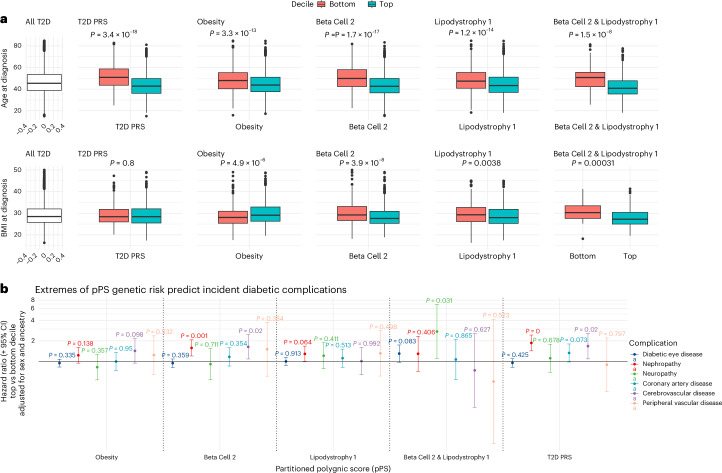
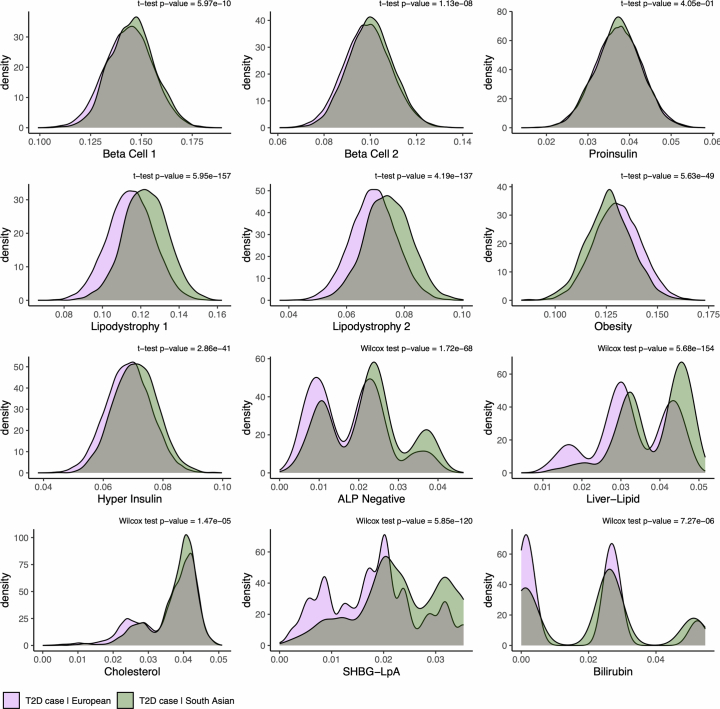
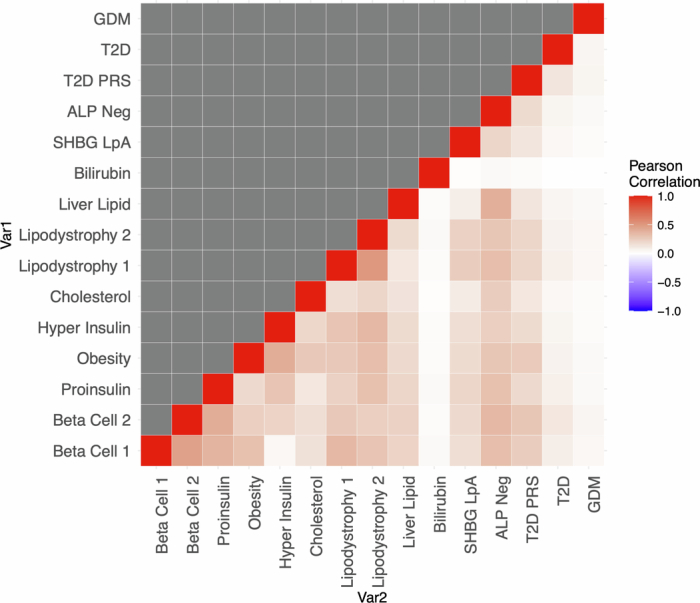
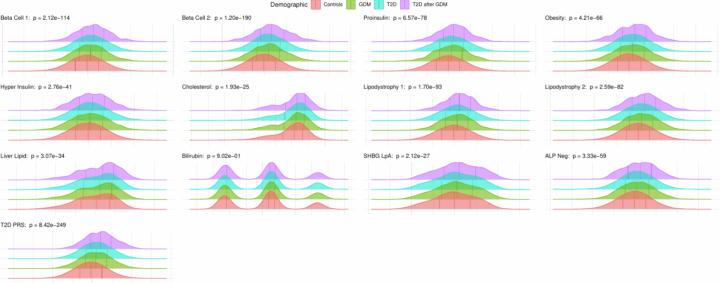
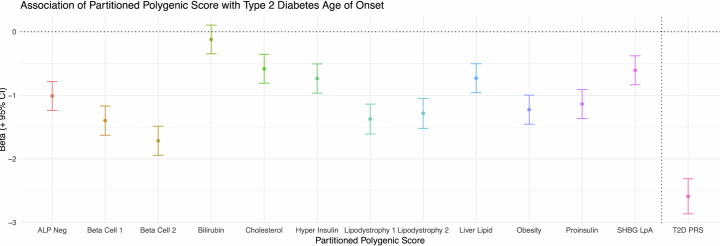
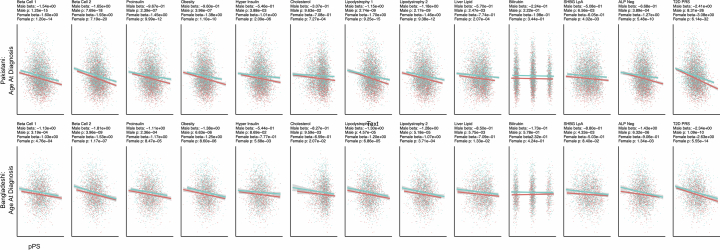
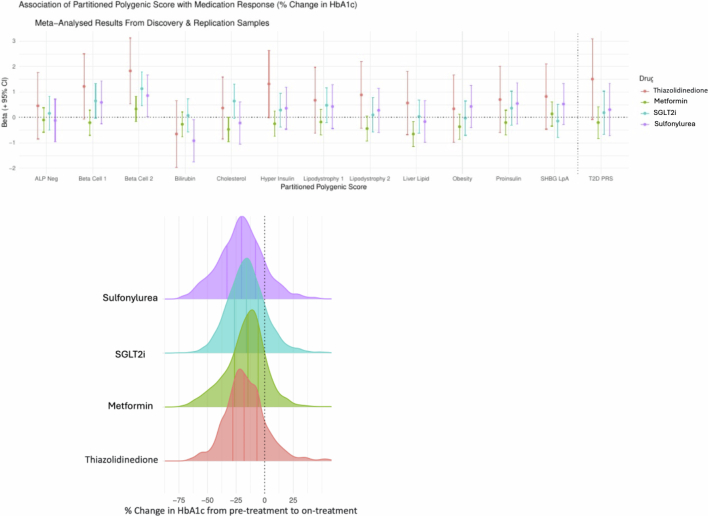
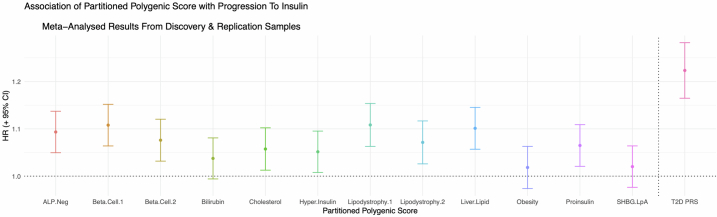
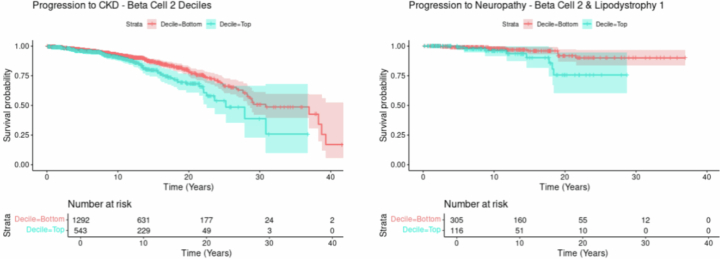
South Asians develop type 2 diabetes (T2D) early in life and often with normal body mass index (BMI). However, reasons for this are poorly understood because genetic research is largely focused on European ancestry groups. We used recently derived multi-ancestry partitioned polygenic scores (pPSs) to elucidate underlying etiological pathways British Pakistani and British Bangladeshi individuals with T2D (n = 11,678) and gestational diabetes mellitus (GDM) (n = 1,965) in the Genes & Health study (n = 50,556). Beta cell 2 (insulin deficiency) and Lipodystrophy 1 (unfavorable fat distribution) pPSs were most strongly associated with T2D, GDM and younger age at T2D diagnosis. Individuals at high genetic risk of both insulin deficiency and lipodystrophy were diagnosed with T2D 8.2 years earlier with BMI 3 kg m-2 lower compared to those at low genetic risk. The insulin deficiency pPS was associated with poorer HbA1c response to SGLT2 inhibitors. Insulin deficiency and lipodystrophy pPSs were associated with faster progression to insulin dependence and microvascular complications. South Asians had a greater genetic burden from both of these pPSs than white Europeans in the UK Biobank. In conclusion, genetic predisposition to insulin deficiency and lipodystrophy in British Pakistani and British Bangladeshi individuals is associated with earlier onset of T2D, faster progression to complications, insulin dependence and poorer response to medication.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures
References
-
- Magliano, D. & Boyko, E. J. IDF Diabetes Atlas (International Diabetes Federation, 2021).
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
