

Outcomes of ED chest pain visits: the prognostic value of negative but measurable high-sensitivity cardiac troponin (hs-cTn) levels
- PMID: 39592937
- PMCID: PMC11600857
- DOI: 10.1186/s12873-024-01128-1
Outcomes of ED chest pain visits: the prognostic value of negative but measurable high-sensitivity cardiac troponin (hs-cTn) levels
Abstract
Background: Chest pain is a common condition in the emergency department (ED). High-sensitivity cardiac troponin (hs-cTn) assays are crucial for diagnosing acute coronary syndrome, but the implications of "negative but measurable" hs-cTn levels are not well understood. This study assesses the outcomes of patients with acute chest pain discharged from the ED based on their hs-cTn levels.
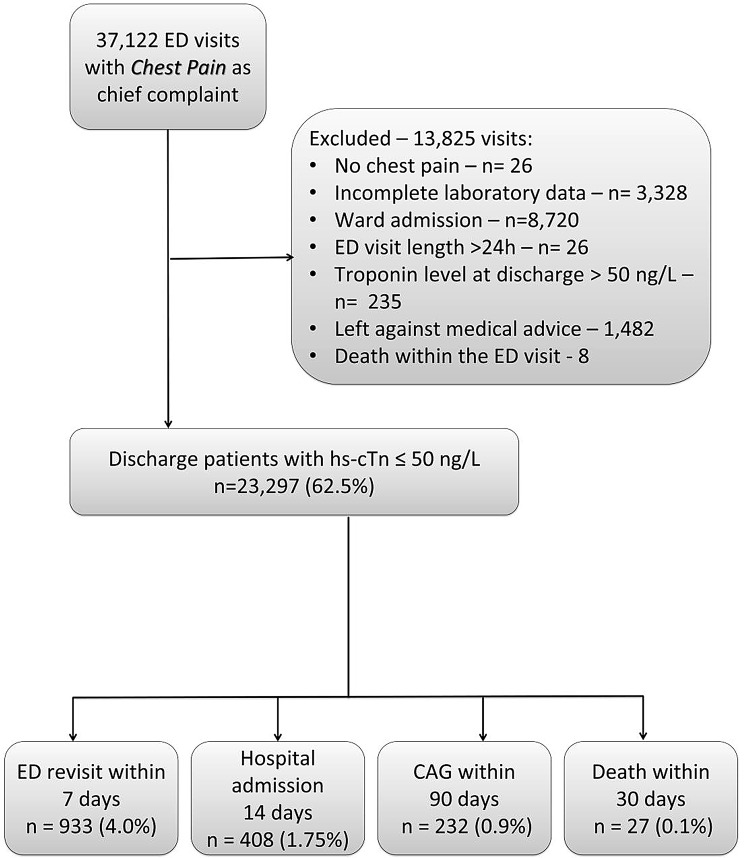
Methods: This retrospective cohort study analyzed medical records of patients aged 18 and older presenting with chest pain to the Tel Aviv Sourasky Medical Center ED from 2017 to 2022. We compared patients with negative but measurable hs-cTn levels (3-50 ng/L) to those with very low hs-cTn levels (< 3 ng/L). Primary outcomes included 90- days coronary angiogram (CAG), and secondary outcomes were 7- days ED revisits, 14-days hospital admissions, and 30- days mortality.
Results: Of 32,162 eligible patients, 23,297 had hs-cTn levels ≤ 50 ng/L. Patients with negative but measurable hs-cTn levels had higher rates of 90-days CAG (1.8% vs. 0.5%, p < 0.001), 7-day ED revisits (5.2% vs. 3.3%, p < 0.001), 14-day hospital admissions (3.1% vs. 0.9%, p < 0.001), and 30-day mortality (0.3% vs. 0.01%, p < 0.001) compared to those with very low hs-cTn levels. Independent predictors for 90 days CAG included age ≥ 57 years, male sex, and hs-cTn ≥ 3.5 ng/L.
Conclusions: Negative but measurable hs-cTn levels are linked to worse outcomes than very low hs-cTn levels in discharged ED patients. Closer follow-up and further cardiac evaluation may be warranted for these patients.
Keywords: Chest pain; ED discharge; Outcomes after discharge; Troponin.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: The study was conducted in accordance with the Declaration of Helsinki and approved by the Tel-Aviv Sourasky Medical Center Institutional Review Board (Study number: TLV-22-0151). The need for consent to participate was waived by an Institutional Review Board. Consent for participate: Not applicable as written informed consent was not necessary because no patient data has been included in the manuscript. The need for consent to participate was waived by an Institutional Review Board (Study number: TLV-22-0151). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Hsia RY, Hale Z, Tabas JA. A national study of the prevalence of life-threatening diagnoses in patients with chest pain. JAMA Intern Med. 2016;176(7):1029–32. - PubMed
-
- Bösner S, Becker A, Haasenritter J, Abu Hani M, Keller H, Sönnichsen AC, et al. Chest pain in primary care: epidemiology and pre-work-up probabilities. Eur J Gen Pract. 2009;15(3):141–6. - PubMed
-
- Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, AHA/ACC/ASE/CHEST et al. /SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2021;78(22):e187-e285. - PubMed
-
- Kane AE, Howlett SE. Differences in cardiovascular aging in men and women. Sex-specific Anal Cardiovasc Function. 2018:1065:389–411. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
