

Epidemiology of healthcare-associated bloodstream infection in South African neonatal units
- PMID: 39593003
- PMCID: PMC11600642
- DOI: 10.1186/s12879-024-10219-0
Epidemiology of healthcare-associated bloodstream infection in South African neonatal units
Abstract
Background: Reports of healthcare-associated bloodstream infection (HA-BSI) epidemiology in African neonatal units are limited.
Methods: We conducted a cross-sectional study (2017-2018) in nine neonatal units in the Western Cape Province, South Africa, including central, regional and district hospitals (416 beds) using laboratory and clinical records. Patient demographics, HA-BSI rates, pathogen spectrum, and hospital outcomes and empiric antibiotic coverage rates were determined.
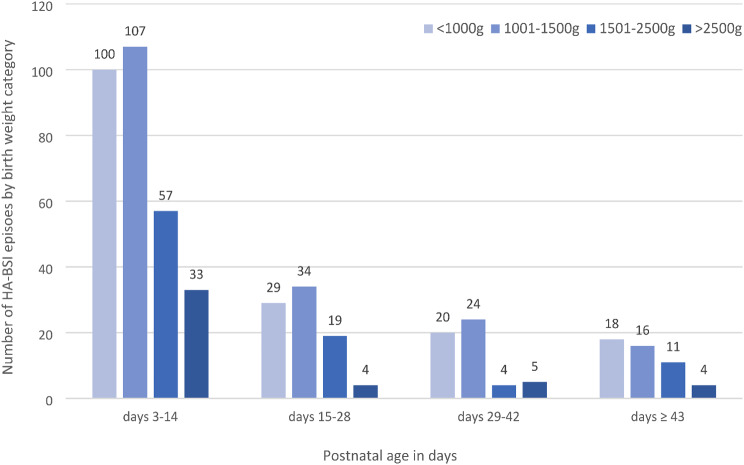
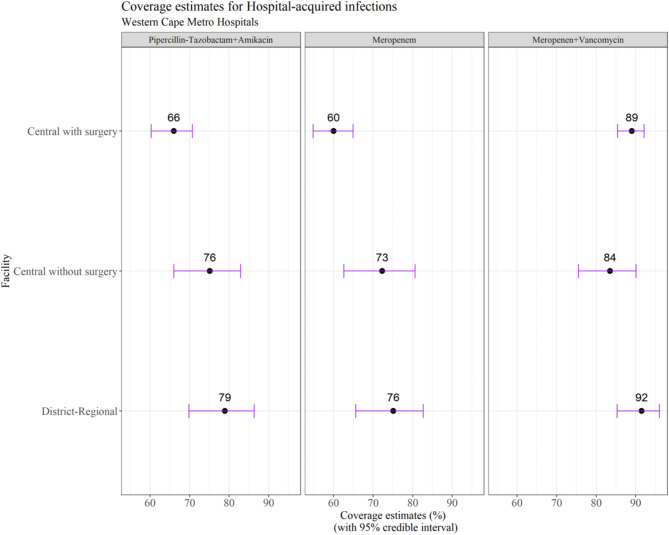
Results: Over two years, 23,748 neonates were admitted with unit occupancy rates ranging from 79 to 93%. 485 HA-BSI episodes occurred, with median onset at 11 (IQR 7-24) days of life. Most HA-BSI episodes (348; 72%) affected very low birth weight neonates (< 1500 g). The overall HA-BSI rate was 2.0/1000 patient days. The highest HA-BSI rate was observed at the central unit with onsite surgery (3.8/1000 patient days). Crude HA-BSI mortality was 31.8% (154/485) with two-thirds of deaths occurring within three days of BSI onset. Higher mortality was observed for Gram-negative/fungal BSI compared to Gram-positive BSI (RR 1.5; 95%CI 1.1-2.0; p = 0.01) and very preterm neonates (gestation < 32 weeks) versus ≥ 32 weeks (RR 1.5; 95%CI 1.1-2.1; p = 0.01). Mean estimated empiric antibiotic coverage rates varied by unit type: 66-79% for piperacillin-tazobactam plus amikacin, 60-76% for meropenem and 84-92% for meropenem plus vancomycin.
Conclusion: Most HA-BSI events affected preterm neonates at the central hospital with onsite surgery. One-third of patients with HA-BSI died, with highest mortality in preterm infants and Gram-negative/fungal BSI. Empiric antibiotic regimens provide moderate coverage of circulating pathogens but require annual review given increasing carbapenem resistance rates.
Keywords: Antimicrobial resistance; Bloodstream infection; Healthcare-associated infection; Hospital-acquired infection; Neonatal intensive care unit; Neonate; Nosocomial; Sepsis.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: The Stellenbosch University Health Research Ethics Committee (SU HREC) and the Tygerberg Hospital management reviewed and approved the study protocol SU HREC approvals (N18/07/068, N20/07/070), in accordance with the Declaration of Helsinki standards. The Stellenbosch University Health Research Ethics Committee (SU HREC) approved a waiver of individual informed consent for the retrospective analysis of neonatal bloodstream infection data. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Early onset neonatal bloodstream infections in South African hospitals.BMC Infect Dis. 2025 Jan 20;25(1):85. doi: 10.1186/s12879-024-10406-z. BMC Infect Dis. 2025. PMID: 39833703 Free PMC article.
-
Bloodstream infections and antimicrobial resistance patterns in a South African neonatal intensive care unit.Paediatr Int Child Health. 2014 May;34(2):108-14. doi: 10.1179/2046905513Y.0000000082. Epub 2013 Dec 6. Paediatr Int Child Health. 2014. PMID: 24621234
-
Trends in paediatric bloodstream infections at a South African referral hospital.BMC Pediatr. 2015 Apr 2;15:33. doi: 10.1186/s12887-015-0354-3. BMC Pediatr. 2015. PMID: 25884449 Free PMC article.
-
Epidemiology and impact of bloodstream infections among kidney transplant recipients: A retrospective single-center experience.Transpl Infect Dis. 2018 Feb;20(1). doi: 10.1111/tid.12815. Epub 2018 Jan 19. Transpl Infect Dis. 2018. PMID: 29151282 Review.
-
Neonatal bloodstream infections.Curr Opin Infect Dis. 2021 Oct 1;34(5):533-537. doi: 10.1097/QCO.0000000000000764. Curr Opin Infect Dis. 2021. PMID: 34261905 Review.
References
-
- United Nations Inter-agency Group for Child Mortality Estimation (UN IGME). Levels & trends in Child Mortality: Report 2022, estimates developed by the United Nations Inter-agency Group for Child Mortality Estimation. New York: United Nations Children’s Fund; 2023.
-
- Levels & Trends in Child Mortality. Report 2020. United Nations Children’s Fund, The (UNICEF); 2020.
-
- Sass L, Karlowicz MG. Healthcare-Associated Infections in the Neonate. Principles and Practice of Pediatric Infectious Diseases. 2018;560-566.e3. doi:10.1016/B978-0-323-40181-4.00094-3
-
- Zingg W, Posfay-Barbe KM, Pittet D. Healthcare-associated infections in neonates. Curr Opin Infect Dis. 2008;21(3):228–34. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
