

Upper Crossed Syndrome and Scapulae Upper-Trapping: A Mesotherapy Protocol in Cervicoscapulobrachial Pain-The 8:1 Block
- PMID: 39593802
- PMCID: PMC11591527
- DOI: 10.3390/bioengineering11111142
Upper Crossed Syndrome and Scapulae Upper-Trapping: A Mesotherapy Protocol in Cervicoscapulobrachial Pain-The 8:1 Block
Abstract
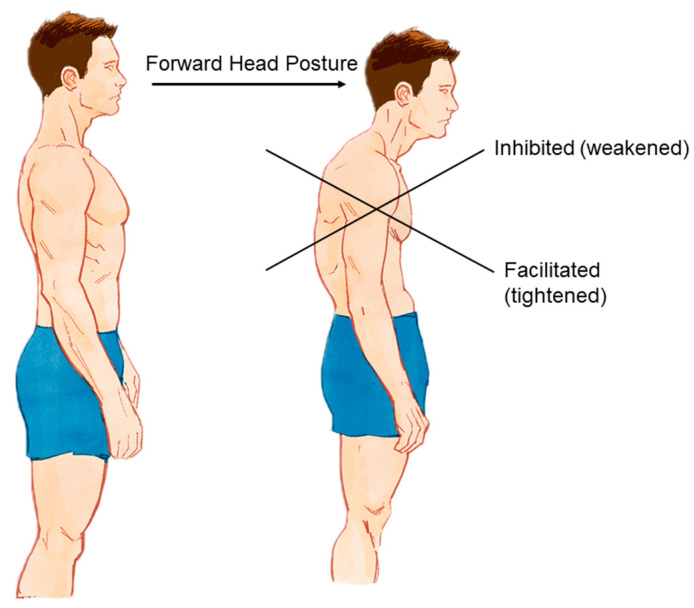
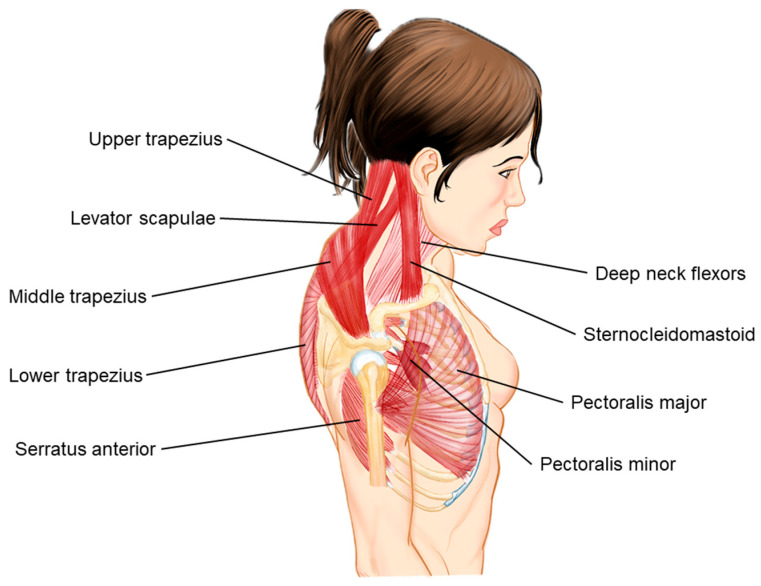
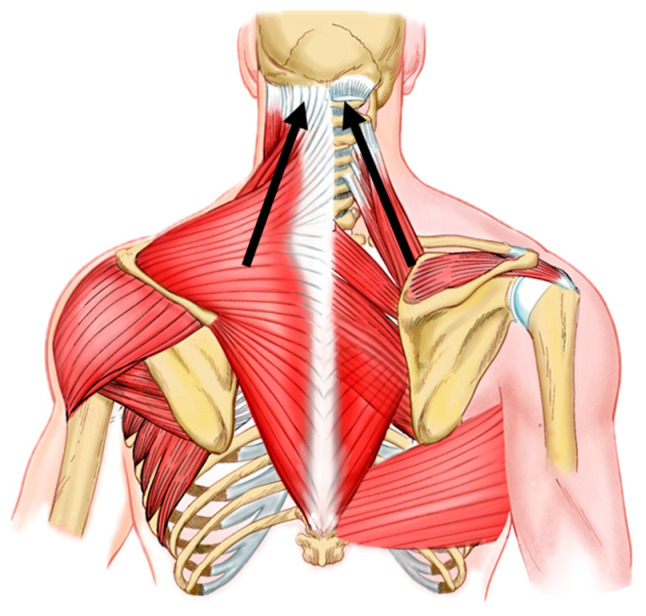
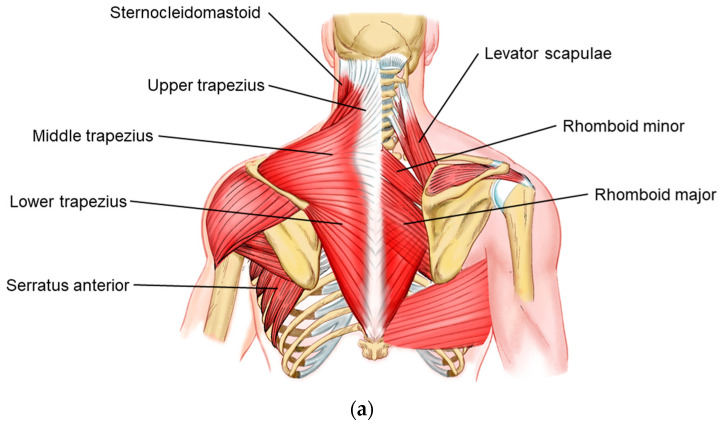
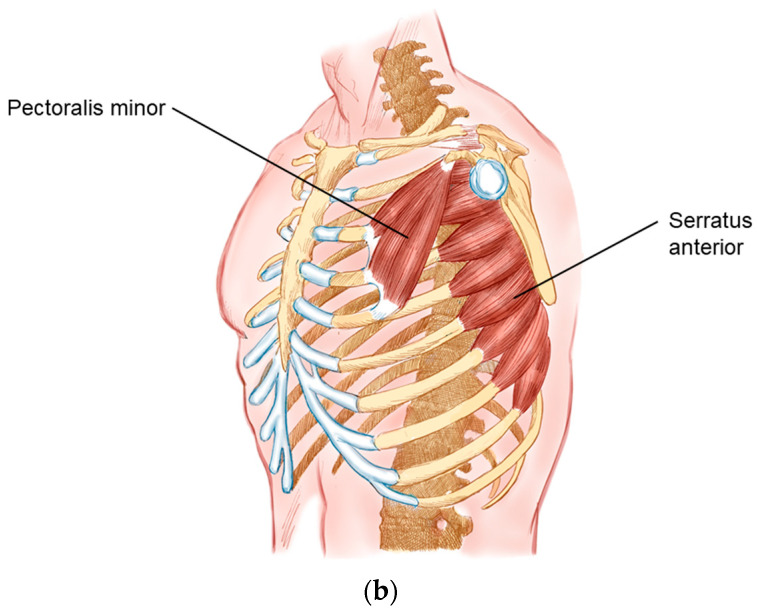
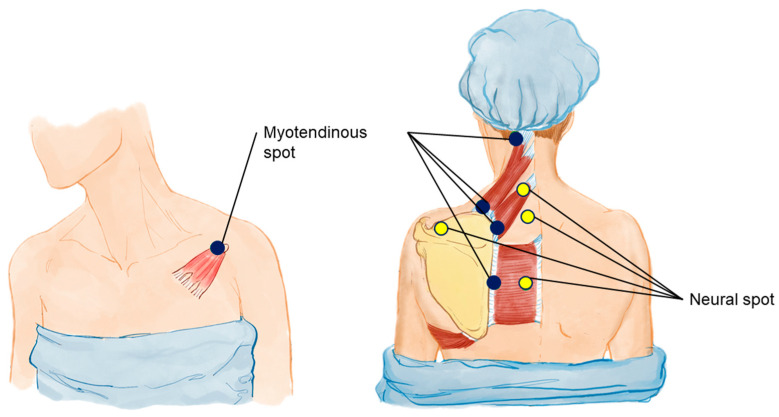
Upper Crossed Syndrome (UCS), described by Vladimir Janda, is characterized by postural changes involving the cervical spine and trunk, leading to biomechanical limitations and cervicoscapulobrachial pain. This study proposes a mesotherapy protocol, termed the 8:1 block, to address cervicoscapulobrachialgia by targeting the scapulae and associated musculature. The scapula, central to shoulder girdle kinematics, often exhibits dyskinesis and muscular imbalances, notably the pattern referred to as scapular upper trapping (SUT). SUT involves scapular elevation, medial rotation, and shoulder protraction, contributing to cervicobrachial pain. The protocol includes a comprehensive assessment of muscle tone changes and biomechanical considerations, highlighting the importance of the scapula in upper limb movement and posture. Key anatomical changes involve tightened upper trapezius, levator scapulae, and pectoralis minor muscles, with weakened middle trapezius and serratus anterior. The mesotherapy approach targets these imbalances through specific injection points to alleviate muscle tension and correct postural deviations. Case studies from our clinic demonstrate the protocol's effectiveness in reducing pain and restoring scapular biomechanics. Patients reported significant improvements in pain relief and functional outcomes, underscoring the clinical utility of the 8:1 block in treating cervicoscapulobrachialgia. This protocol offers a feasible, cost-effective intervention that enhances the efficacy of traditional therapeutic exercises by addressing underlying muscular and biomechanical dysfunctions. In conclusion, the 8:1 block mesotherapy protocol provides a novel approach to managing cervicoscapulobrachial pain by focusing on scapular biomechanics and muscle tension. Further studies are needed to validate these findings and refine the protocol for broader clinical application.
Keywords: cervicoscapulobrachialgia; mesotherapy protocol; scapular dyskinesis; scapular upper trapping; upper crossed syndrome.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Effects of scapular retraction/protraction position and scapular elevation on shoulder girdle muscle activity during glenohumeral abduction.Hum Mov Sci. 2019 Apr;64:55-66. doi: 10.1016/j.humov.2019.01.005. Epub 2019 Jan 16. Hum Mov Sci. 2019. PMID: 30660072
-
Effects of Crossed Brassiere Straps on Pain, Range of Motion, and Electromyographic Activity of Scapular Upward Rotators in Women With Scapular Downward Rotation Syndrome.PM R. 2015 Dec;7(12):1261-1268. doi: 10.1016/j.pmrj.2015.05.016. Epub 2015 May 29. PM R. 2015. PMID: 26032346 Clinical Trial.
-
Relationship between scapular elevation exercises with different alignments and activity of the trapezius and levator scapulae muscles.J Phys Ther Sci. 2023 Nov;35(11):751-756. doi: 10.1589/jpts.35.751. Epub 2023 Nov 1. J Phys Ther Sci. 2023. PMID: 37915451 Free PMC article.
-
Three-dimensional scapular orientation and muscle activity at selected positions of humeral elevation.J Orthop Sports Phys Ther. 1996 Aug;24(2):57-65. doi: 10.2519/jospt.1996.24.2.57. J Orthop Sports Phys Ther. 1996. PMID: 8832468 Review.
-
Kinematic patterns in normal and degenerative shoulders. Part II: Review of 3-D scapular kinematic patterns in patients with shoulder pain, and clinical implications.Ann Phys Rehabil Med. 2018 Jan;61(1):46-53. doi: 10.1016/j.rehab.2017.09.002. Epub 2017 Oct 5. Ann Phys Rehabil Med. 2018. PMID: 28987866 Review.
References
-
- Janda V. Janda Compendium. Volume II. O.P.T.P.; Plymouth, MN, USA: 1997. pp. 7–13.
-
- Schwartz L. A resume, with comments, of the available literature relating to posture. Public Health Rep. 1927;42:1219–1224. doi: 10.2307/4578305. - DOI
-
- Iannotti J.P., Parker R.D. The Netter Collection of Medical Illustrations (Frank H. Netter, MD). Musculoskeletal System, Part 1: Upper Limb. 2nd ed. Elsevier; Amsterdam, The Netherlands: 2013. pp. 2–3.
LinkOut - more resources
Full Text Sources
