

Primary Osteoporosis Induced by Androgen and Estrogen Deficiency: The Molecular and Cellular Perspective on Pathophysiological Mechanisms and Treatments
- PMID: 39596206
- PMCID: PMC11593909
- DOI: 10.3390/ijms252212139
Primary Osteoporosis Induced by Androgen and Estrogen Deficiency: The Molecular and Cellular Perspective on Pathophysiological Mechanisms and Treatments
Abstract
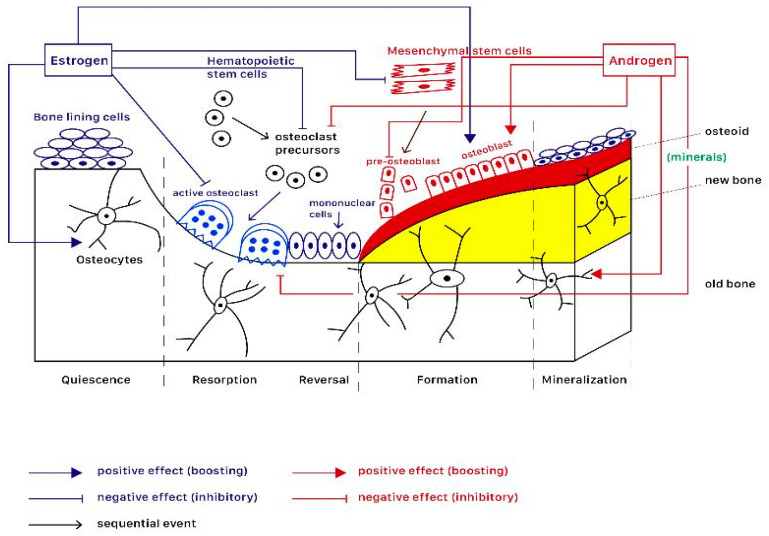
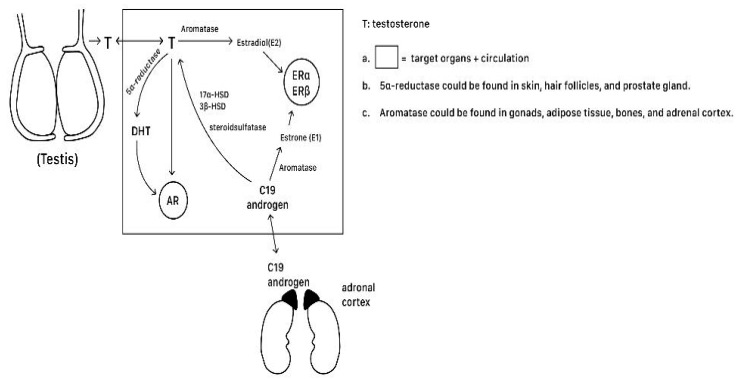
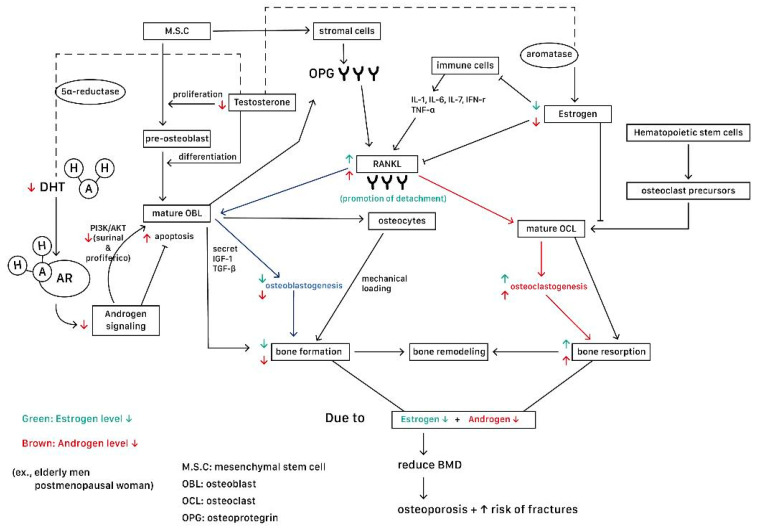
Primary osteoporosis is closely linked to hormone deficiency, which disrupts the balance of bone remodeling. It affects postmenopausal women but also significantly impacts older men. Estrogen can promote the production of osteoprotegerin, a decoy receptor for RANKL, thereby preventing RANKL from activating osteoclasts. Furthermore, estrogen promotes osteoblast survival and function via activation of the Wnt signaling pathway. Likewise, androgens play a critical role in bone metabolism, primarily through their conversion to estrogen in men. Estrogen deficiency accelerates bone resorption through a rise in pro-inflammatory cytokines (IL-1, IL-6, TNF-α) and RANKL, which promote osteoclastogenesis. In the classic genomic pathway, estrogen binds to estrogen receptors in the cytoplasm, forming a complex that migrates to the nucleus and binds to estrogen response elements on DNA, regulating gene transcription. Androgens can be defined as high-affinity ligands for the androgen receptor; their combination can serve as a ligand-inducible transcription factor. Hormone replacement therapy has shown promise but comes with associated risks and side effects. In contrast, the non-genomic pathway involves rapid signaling cascades initiated at the cell membrane, influencing cellular functions without directly altering gene expression. Therefore, the ligand-independent actions and rapid signaling pathways of estrogen and androgen receptors can be harnessed to develop new drugs that provide bone protection without the side effects of traditional hormone therapies. To manage primary osteoporosis, other pharmacological treatments (bisphosphonates, teriparatide, RANKL inhibitors, sclerostin inhibitors, SERMs, and calcitonin salmon) can ameliorate osteoporosis and improve BMD via actions on different pathways. Non-pharmacological treatments include nutritional support and exercise, as well as the dietary intake of antioxidants and natural products. The current study reviews the processes of bone remodeling, hormone actions, hormone receptor status, and therapeutic targets of primary osteoporosis. However, many detailed cellular and molecular mechanisms underlying primary osteoporosis seem complicated and unexplored and warrant further investigation.
Keywords: Wnt signaling pathway; androgen; estrogen; osteoporosis; osteoprotegerin.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Osteoporosis Due to Hormone Imbalance: An Overview of the Effects of Estrogen Deficiency and Glucocorticoid Overuse on Bone Turnover.Int J Mol Sci. 2022 Jan 25;23(3):1376. doi: 10.3390/ijms23031376. Int J Mol Sci. 2022. PMID: 35163300 Free PMC article. Review.
-
Hormone-Related and Drug-Induced Osteoporosis: A Cellular and Molecular Overview.Int J Mol Sci. 2023 Mar 18;24(6):5814. doi: 10.3390/ijms24065814. Int J Mol Sci. 2023. PMID: 36982891 Free PMC article. Review.
-
Interaction between bone and immune cells: Implications for postmenopausal osteoporosis.Semin Cell Dev Biol. 2022 Mar;123:14-21. doi: 10.1016/j.semcdb.2021.05.014. Epub 2021 May 20. Semin Cell Dev Biol. 2022. PMID: 34024716 Review.
-
Prevention and treatment of postmenopausal osteoporosis.J Steroid Biochem Mol Biol. 2014 Jul;142:155-70. doi: 10.1016/j.jsbmb.2013.09.008. Epub 2013 Oct 29. J Steroid Biochem Mol Biol. 2014. PMID: 24176761 Free PMC article. Review.
-
Siglec-15 is a potential therapeutic target for postmenopausal osteoporosis.Bone. 2015 Feb;71:217-26. doi: 10.1016/j.bone.2014.10.027. Epub 2014 Nov 8. Bone. 2015. PMID: 25460183
Cited by
-
Sex differences in drug-induced osteoporosis: a pharmacovigilance study based on the FAERS database.Front Public Health. 2025 Jul 24;13:1630412. doi: 10.3389/fpubh.2025.1630412. eCollection 2025. Front Public Health. 2025. PMID: 40777658 Free PMC article.
-
The link between osteoporosis and cardiovascular diseases: a review of shared mechanisms, risk factors, and therapeutic approaches.Osteoporos Int. 2025 Jul;36(7):1129-1142. doi: 10.1007/s00198-025-07553-7. Epub 2025 Jun 2. Osteoporos Int. 2025. PMID: 40455217 Review.
-
Vertebral Osteoporosis in Systemic Lupus Erythematosus: A Possible Involvement of Inflammation-Related Osteoblast Ferroptosis.J Inflamm Res. 2025 Apr 25;18:5587-5599. doi: 10.2147/JIR.S523051. eCollection 2025. J Inflamm Res. 2025. PMID: 40303004 Free PMC article.
-
Hormonal Contraception and Bone Metabolism: Emerging Evidence from a Systematic Review and Meta-Analysis of Studies on Post-Pubertal and Reproductive-Age Women.Pharmaceuticals (Basel). 2025 Jan 8;18(1):61. doi: 10.3390/ph18010061. Pharmaceuticals (Basel). 2025. PMID: 39861124 Free PMC article. Review.
References
-
- International Osteoporosis Foundation Guidance for Policy Shaping. [(accessed on 10 August 2024)]. Available online: https://www.osteoporosis.foundation/sites/iofbonehealth/files/2021-03/Gu....
-
- International Osteoporosis Foundation Epidemiology of Osteoporosis and Fragility Fractures. [(accessed on 25 July 2024)]. Available online: https://www.osteoporosis.foundation/facts-statistics/epidemiology-of-ost....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
