

An Intraoperative Ultrasound Evaluation of Axillary Lymph Nodes: Cassandra Predictive Models in Patients with Breast Cancer-A Multicentric Study
- PMID: 39596991
- PMCID: PMC11596888
- DOI: 10.3390/medicina60111806
An Intraoperative Ultrasound Evaluation of Axillary Lymph Nodes: Cassandra Predictive Models in Patients with Breast Cancer-A Multicentric Study
Abstract
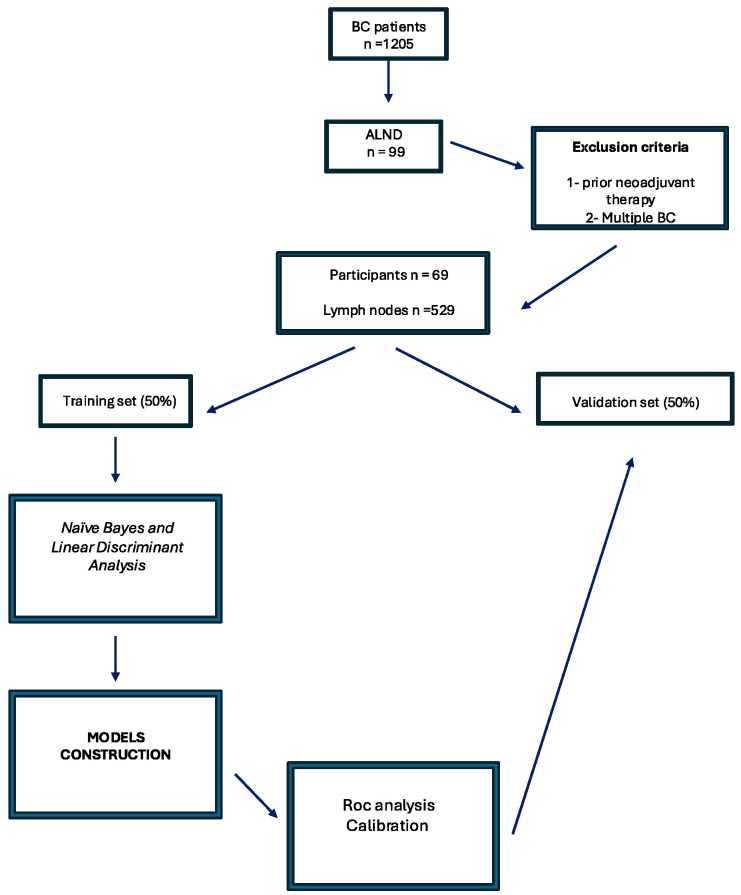
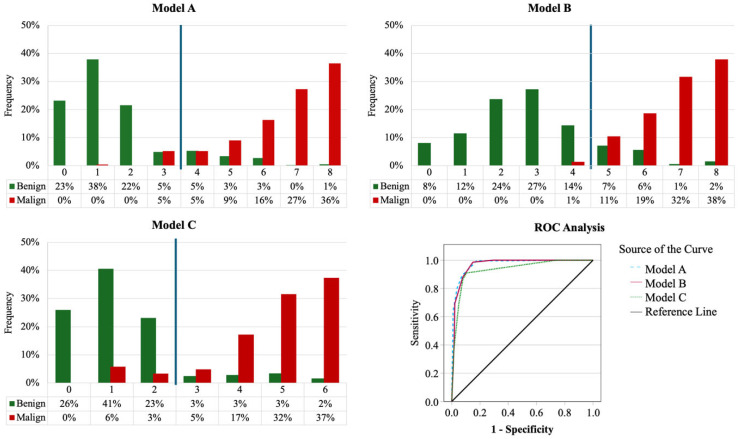
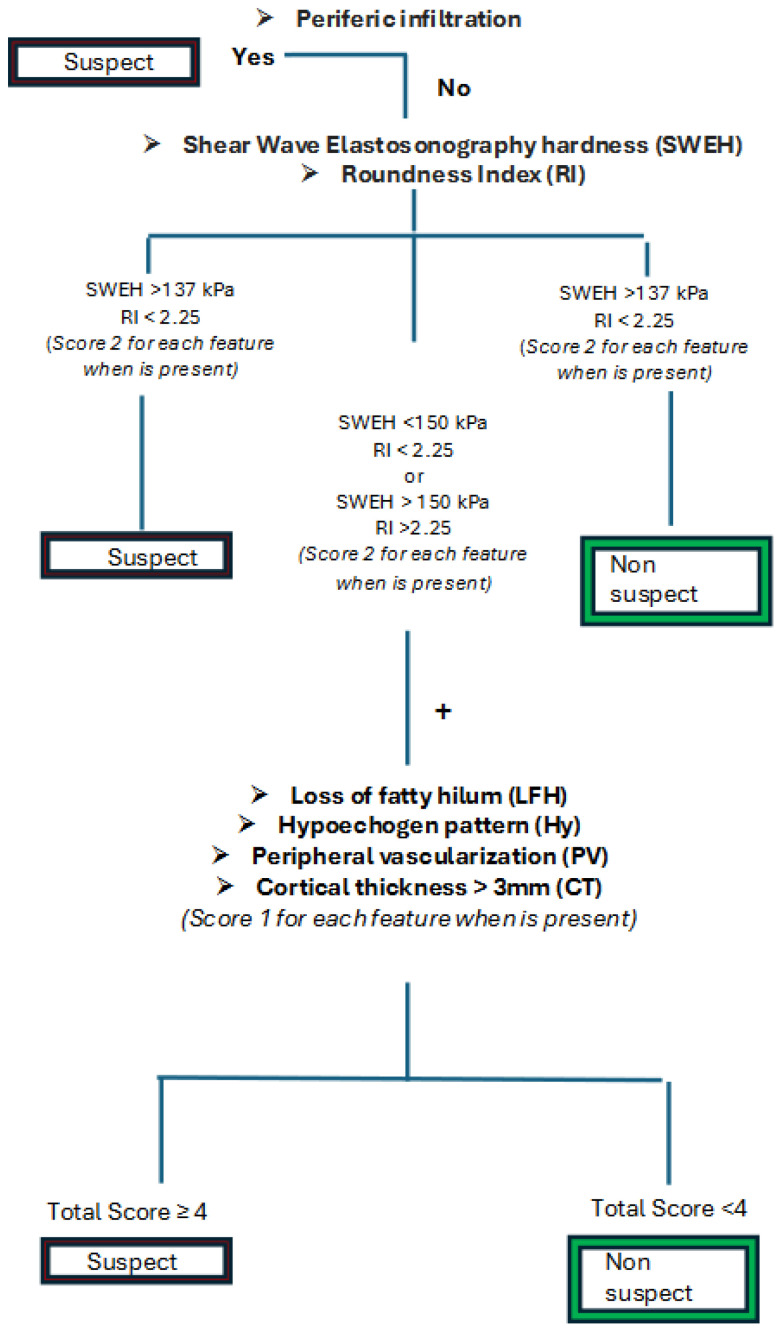
Background and Objectives: Axillary lymph node (ALN) staging is crucial for the management of invasive breast cancer (BC). Although various radiological investigations are available, ultrasound (US) is the preferred tool for evaluating ALNs. Despite its immediacy, widespread use, and good predictive value, US is limited by intra- and inter-operator variability. This study aims to evaluate US and Elastosonography Shear Wave (SW-ES) parameters for ALN staging to develop a predictive model, named the Cassandra score (CS), to improve the interpretation of findings and standardize staging. Materials and Methods: Sixty-three women diagnosed with BC and treated at two Italian hospitals were enrolled in the study. A total of 529 lymph nodes were surgically removed, underwent intraoperative US examination, and were individually sent for a final histological analysis. The study aimed to establish a direct correlation between eight US-SWES features (margins, vascularity, roundness index (RI), loss of hilum fat, cortical thickness, shear-wave elastography hardness (SWEH), peripheral infiltration (PI), and hypoechoic appearance) and the histological outcome (benign vs. malignant). Results: Several statistical models were compared. PI was strongly correlated with malignant ALNs. An ROC analysis for Model A revealed an impressive AUC of 0.978 (S.E. = 0.007, p < 0.001), while in Model B, the cut-offs of SWEH and RI were modified to minimize the risk of false negatives (AUC of 0.973, S.E. = 0.009, p < 0.001). Model C used the same cut-offs as Model B, but excluded SWEH from the formula, to make the Cassandra model usable even if the US machine does not have SW-ES capability (AUC of 0.940, S.E. = 0.015, p < 0.001). A two-tiered model was finally set up, leveraging the strong predictive capabilities of SWEH and RI. In the first tier, only SWES and RI were evaluated: a positive result was predicted if both hardness and roundness were present (SWES > 137 kPa and RI < 1.55), and conversely, a negative result was predicted if both were absent (SWES < 137 kPa and RI > 1.55). In the second tier, if there was a mix of the results (SWES > 137 kPa and RI > 1.55 or SWES < 137 kPa and RI < 1.55), the algorithm in Model B was applied. The model demonstrated an overall prediction accuracy of 90.2% in the training set, 87.5% in the validation set, and 88.9% across the entire dataset. The NPV was notably high at 99.2% in the validation set. This model was named the Cassandra score (CS) and is proposed for the clinical management of BC patients. Conclusion: CS is a simple, non-invasive, fast, and reliable method that showed a PPV of 99.1% in the malignancy prediction of ALNs, potentially being also well suited for young sonographers.
Keywords: axillary staging; axillary surgery; axillary ultrasound; breast cancer; ultrasound score.
Conflict of interest statement
All authors declare no personal conflicts of interest, and no financial support from the companies that produce and/or distribute the drugs, devices, or materials described in this report.
Figures
References
-
- Cardoso F., Kyriakides S., Ohno S., Penault-Llorca F., Poortmans P., Rubio I.T., Zackrisson S., Senkus E., ESMO Guidelines Committee Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019;30:1194–1220. doi: 10.1093/annonc/mdz173. - DOI - PubMed
-
- Fisher E.R., Costantino J., Fisher B., Redmond C. Pathologic findings from the National Surgical Adjuvant Breast Project (Protocol 4). Discriminants for 15-year survival. National Surgical Adjuvant Breast and Bowel Project Investigators. Cancer. 1993;71:2141–2150. doi: 10.1002/1097-0142(19930315)71:6+<2141::AID-CNCR2820711603>3.0.CO;2-F. - DOI - PubMed
-
- Veronesi U., Paganelli G., Viale G., Luini A., Zurrida S., Galimberti V., Intra M., Veronesi P., Robertson C., Maisonneuve P., et al. A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer. N. Engl. J. Med. 2003;349:546–553. doi: 10.1056/NEJMoa012782. - DOI - PubMed
-
- Del Bianco P., Zavagno G., Burelli P., Scalco G., Barutta L., Carraro P., Pietrarota P., Meneghini G., Morbin T.G., Pecoraro P., et al. Morbidity comparison of sentinel lymph node biopsy versus conventional axillary lymph node dissection for breast cancer patients: Results of the sentinella-GIVOM Italian randomised clinical trial. Eur. J. Surg. Oncol. 2008;34:508–513. doi: 10.1016/j.ejso.2007.05.017. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
